Combination Regimens for Metastatic Melanoma
A number of new combination approaches have gained approval in the past year for the treatment of patients with BRAF-mutant metastatic melanoma, expanding the number of effective treatment options that can improve quality and length of life for many patients.
BRAF-mutant metastatic melanoma, expanding the number of effective treatment options that can improve quality and length of life for many patients.
Although single-agent therapy with targeted inhibitors of the BRAF kinase yields initial high response rates and a proven survival benefit, approximately half of all patients relapse after 6 to 7 months due to acquired resistance. The underlying escape mechanisms are complex and dynamic and involve reactivation of the mitogen-activated protein kinase (MAPK) pathway through genetic changes affecting BRAF, RAS, and MEK kinase activity, epigenetic changes, and immune evasion.1,2
Concomitant inhibition of both BRAF and MEK kinases with targeted inhibitors has become, “The recommend approach for molecularly targeted therapy,” according to Keith T. Flaherty, MD, with Massachusetts General Hospital Cancer Center, in Boston, Massachusetts.

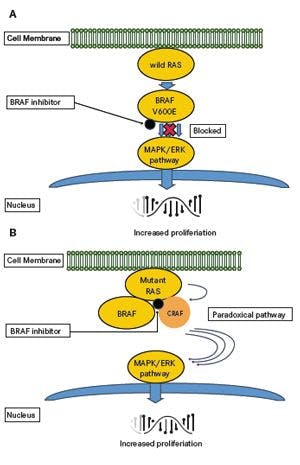
Role of BRAF inhibition in the MAP kinase pathway
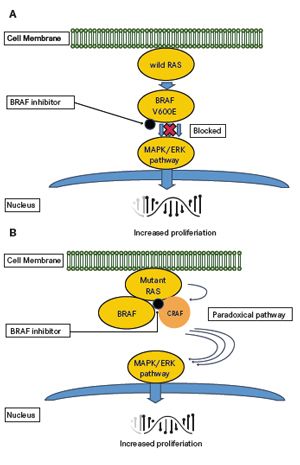
A.When BRAF kinase is constitutively activated due to a mutation (eg, V600E), treatment with BRAF inhibitors results in blockade of downstream MAPK pathway.B.In cells with wild-type BRAF, treatment with BRAF inhibitors results in transactivation of CRAF and promotion of RAF dimerization, causing paradoxical activation of downstream MAPK pathway in the presence of upstream oncogenic changes, such as RAS mutations.
The rationale for combining BRAF and MEK inhibition is to delay resistance associated with the reactivation of MEKERK signalling after single-agent BRAF inhibition. Upfront inhibition of both BRAF and MEK kinases can delay emergence of treatment resistance and decrease the incidence of cutaneous hyperproliferative lesions associated with the paradoxical activation of the MAPK pathway following BRAF inhibitor monotherapy.3
“There are two bases for adding a MEK inhibitor to a BRAF inhibitor,” said Flaherty. “One related to overcoming resistance and the other to countering a mechanism of toxicity.”
Combined BRAF-MEK Inhibition: Dabrafenib/ Trametinib
Based on data from two phase III studies demonstrating overall survival (OS) prolongation, the dabrafenib/trametinib combination regimen received full FDA approval for the treatment of patients with unresectable or metastaticBRAF-mutated melanoma in November 2015.
The most recent analysis from the COMBI-v study presented at the 2015 European Cancer Congress (ECC) reported a 7.6-month prolongation of OS with dabrafenib and trametinib compared with single-agent vemurafenib (25.6 vs 18.0 months; HR, 0.66; 95% CI, 0.53-0.81;P<.001).4The estimated 2-year OS rate was 51% with dabrafenib and trametinib compared with 38% with vemurafenib monotherapy.
COMBI-v was a two-arm, open-label phase III study comparing dabrafenib/trametinib (150 mg twice daily/2 mg once daily) or vemurafenib (960 mg twice daily) in patients withBRAFV600E/K mutation-positive unresectable or metastatic melanoma (n = 704). The study was stopped early in July 2014 following the demonstration of benefit at an interim analysis (P<.0214).5,6
COMBI-v was the second study to demonstrate superiority for the BRAF/MEK inhibitor combination therapy over monotherapy in advanced melanoma. Final OS data from the COMBI-d trial, which had been initiated concomitantly and randomized 423 patients withBRAFV600E/K-mutant melanoma to receive dabrafenib with trametinib (n = 211) or placebo (n = 212), reported a median OS of 25.1 months with the combination compared with 18.7 months with dabrafenib alone (HR, 0.71; 95% CI, 0.55-0.92;P= .011). The 2-year OS rate with the combination was 51% versus 42% with single-agent dabrafenib.5,6
According to Caroline Robert, MD, PhD, lead author of the COMBI-v study, “Dabrafenib plus trametinib has demonstrated superiority over BRAF inhibitor monotherapy now in two phase III trials, supporting its use as a standard-of-care therapy in patients withBRAFV600mutant melanoma.”
Updated analyses from both trials also demonstrate increasing OS advantages of combination therapy over time. In the COMBI-v study, the absolute OS difference increased from 9% at 1 year, to 10% at 18 months, and to 13% at 2 years,4 and in the COMBI-d study from 6% at 1 year to 9% at 2 years.6
In both studies, the addition of MEK inhibition significantly increased the likelihood of having an objective response (ORR; COMBI-d 69% vs 53% for BRAF inhibitor monotherapy,P= .0014; COMBI-v, 66% vs 53%;P= .0008), and more patients achieved complete responses (CR; COMBI-d, 16% vs 13%; COMBI-v, 17% vs 10%). Combination therapies also resulted in longer median duration of response (DoR; COMBI-d, 12.9 vs 10.6 months; COMBI-v, 13.8 vs 8.5 months).4,6
Updated analyses of progression-free survival (PFS), the primary endpoint of the COMBI-v study, showed a significant prolongation with the combination (12.6 vs 7.3 months; HR, 0.61; 95% CI, 0.51-0.73,P<.001), which according to Robert “is the longest achieved in a randomized study for patients with theBRAFV600 mutation to date.”4
The dabrafenib/trametinib combination was associated with fewer adverse events (AE) compared with dabrafenib monotherapy.3,4Importantly, both studies confirmed that combination therapy reduced the incidence of oncogenic toxic effects related to MAPK pathway activation following BRAF inhibitor monotherapy.3,4Cutaneous toxicities including hyperkeratosis (6% vs 33%) and cutaneous squamous carcinoma (3% vs 9%) were less common in the dabrafenib/trametinib group than in the dabrafenib monotherapy group.6 Similarly, in COMBI-v, cutaneous squamous-cell carcinoma and keratoacanthoma were observed in 1% of patients in the combination-therapy group but in 18% in the vemurafenib group.7
The most common AE associated with BRAF/MEK inhibition in both studies was pyrexia (52% and 53% in COMBI-v and COMBI-d, respectively).6,7
Patients of the COMBI-v dabrafenib and trametinib treatment arm showed statistically significant and clinically meaningful improvements in health-related quality of life compared with patients on vemurafenib monotherapy, with improvements in overall health, physical and social functioning, and specific symptoms such as pain, insomnia, and loss of appetite.8
BRAF/MEK inhibitor combinations have emerged as “the new standard of care in terms of targeted agents for melanoma,” said Rene Gonzalez, MD, with the University of Colorado Melanoma Research Clinics. “All three of those studies were positive in the sense that it without a doubt showed that combination therapy is better than single-agent BRAF inhibitor. The overall survival is in the range of two years. The combination progression-free survival is 11 to 12 months, which is better than a single-agent BRAF inhibitor. I can barely think of a role for when a patient would receive just BRAF or MEK inhibitor alone.”
Combined BRAF-MEK Inhibition: Vemurafenib andCobimetinib
The combination of vemurafenib and cobimetinib received FDA approval in November 2015, based on significant prolongation of PFS shown in the phase III coBRIM trial for previously untreated patients (n = 495) withBRAFV600 mutation-positive unresectable locally advanced or metastatic melanoma.9,10
Updated analyses confirmed previously reported clinical benefits from adding cobimetinib (60 mg once daily on days 1-21 of a 28-day cycle) to continuous vemurafenib (960 mg twice daily), which resulted in significant prolongation of PFS (median, 12.3 vs 7.2 months; HR, 0.56; 95% CI, 0.45-0.70;P<.001) and higher probability of response (ORR; 69.6% vs 50%;P<.001), including CR (16% vs 11%) compared with vemurafenib monotherapy.10The median DoR was 12.98 versus 9.23 months, with cobimetinib and placebo, respectively.
Overall survival data after a median of 18.5 months were presented at the 2015 Society for Melanoma Research Congress and revealed OS prolongation of 4.9 months with the combination (median OS, 23.3 vs 17.4 months, combination and vemurafenib alone, respectively; HR, 0.70; 95% CI, 0.55-0.90;P= .005).11The OS rates at 17 months were 65% versus 50% and after 2 years the rates were 48% and 38%, for the combination and single-agent, respectively.10,11
The presenting author Victoria Atkinson, MD, of the Princess Alexandra Hospital in Queensland, Australia, reported: “The benefit of the combination was seen in all subgroups assessed, including ECOG performance status, LDH level, and presence of V600E or V600K mutations.”11
Unique AEs of the vemurafenib/cobimetinib regimen include phototoxicity, including photosensitivity and central serous retinopathy, which were observed in 28% and 20% of patients.10 Other AE more commonly observed with the combination were diarrhea (57% vs 28%), nausea or vomiting (39% vs 24% and 21% vs 12%, respectively), elevated liver enzyme levels (ALT, 24% vs 18%; AST, 22% vs 13%), and an increased creatine kinase level (30% vs 3%).10
Similar to observations with dabrafenib and trametinib, combined BRAF/MEK inhibition was associated with fewer cutaneous toxicities than BRAF inhibitor monotherapy, including hyperkeratosis (10% vs 29%), cutaneous squamous cell carcinomas (3% vs 11%), and keratoacanthomas (<1% vs 8%). Also less frequent were joint pain (33% vs 40%) and hair loss (14% vs 29%).10
Combination Immunotherapy: Nivolumab/Ipilimumab
Dual checkpoint blockade with a combination regimen of the CTLA-4 inhibitor ipilimumab and anti-PD-1 agent nivolumab continues to demonstrate efficacy in advanced melanoma. The combination regimen received accelerated approval for the frontline treatment of patients withBRAFwild-type unresectable or metastatic melanoma in October 2015, based on improved PFS and ORR shown in the phase II CheckMate-069 and phase III CheckMate-067 studies, with expansion of the indication in January 2016 to include patients withBRAFV600 mutation-positive tumors.12,13
Recently reported exploratory data from the 2-year follow-up of the phase II CheckMate-069 trial indicate an OS benefit with the combination.14The 2-year OS rate with first-line combination ipilimumab plus nivolumab therapy (3mg/kg and 1mg/kg, respectively) was 64% versus 54% with nivolumab alone.14Across the entire study population (n = 142), which included patients withBRAFmutant melanoma (n = 33), median OS had not been reached in either treatment group.
Patients with BRAF wild-type melanoma receiving the combination (n = 72) had a 42% OS improvement compared with ipilimumab monotherapy. Median OS had not been reached and was 24.8 months with ipilimumab monotherapy (HR, 0.58; 95% CI, 0.31-1.08). Two-year OS rates were 69% versus 53% with the combination and monotherapy, respectively.14
According to lead author Michael Postow, MD, with Memorial Sloan Kettering Cancer Center, New York, high survival rates in the ipilimumab monotherapy arm were related to a large amount of crossover to other agents, including PD-1 agents, at progression.14OS results from the double-blind phase III CheckMate-067 study are pending.
Combination immunotherapy with ipilimumab/nivolumab capitalizes on non-redundant mechanisms of action of CTLA-4 and PD-1 inhibition that may result in synergistic effects. Specifically, ipilimumab blockade of CTLA-4 augments T-cell activation and proliferation, whereas nivolumab-mediated suppression of PD-1 activity restores the active T-cell response within the tumor microenvironment.
Outcomes from CheckMate-067 trial (n = 945 patients with bothBRAFV600 mutant and wild-type advanced melanoma) have shown that first-line nivolumab alone or in combination with ipilimumab doubled the median time to disease progression compared with ipilimumab monotherapy (median PFS, 11.5 months for the combination, 6.9 months for nivolumab monotherapy, and 2.9 months for ipilimumab monotherapy).12 Compared with ipilimumab monotherapy, the combination regimen and nivolumab monotherapy were associated with 58% and 43% reduction in the risk of disease progression, respectively (HR, 0.42;P<.0001 and HR, 0.57;P<.0001, respectively).12
Two-year assessment data from the phase II CheckMate-069 study showed similar findings. Among all randomized patients, median PFS had also not been reached in the combination treatment arm and was 3.0 months with ipilimumab monotherapy (HR, 0.36;P<.0001), which according to Postow “reflects a 64% reduction in the hazard of progression or death in this all-randomized patient population, which is very impressive and statistically significant.”14
Ipilimumab/nivolumab combination therapy has produced ORRs of up to 61% among patients withBRAFwild-type tumors in the CheckMate-069 study,13and 50% in the phase III CheckMate-067 study,12including 22% and 11.5% complete responses, respectively, all of which were significantly higher than those with ipilimumab monotherapy (ORR, 11% and 14%, respectively; CR, 0% and 7%, respectively).12,13
In both studies, the combination regimen delivered rapid and durable responses, with time to response of 2.9 to 2.7 months.12,13 At the 2-year follow-up of the CheckMate-067 study, the median DoR was not reached in either arm, and 80% of responses to the combination (45 of 56) and ipilimumab monotherapy (4 of 5) were ongoing.14Median tumor burden by RECIST v1.1 decreased by 70% and 51% in patients on dual inhibitor therapy in CheckMate-069 and -67, respectively, but increased by 5% and 5.9% among patients receiving ipilimumab only (TABLE 1).12,14
TABLE 1. Efficacy of Frontline Combination Regimens inBRAF-mutant Melanoma
ORR
median PFS, months
median OS, months
2-year OS rate
COMBI-v (dabrafenib/trametinib)
66%
12.6
26.6
51%
COMBI-d (dabrafenib/trametinib)
69%
11.0
25.1
51%
coBRIM (vemurafenib/cobimetinib)
70%
12.3
23.3
48%
CheckMate-069 (ipilimumab/nivolumab)
52%
8.5
NR
NR
CheckMate-067 (ipilimumab/nivolumab)
NR
11.7
NR
NR
Because of substantially increased toxicities, the nivolumab/ipilimumab combination requires careful patient selection. In CheckMate-067, grade 3/4 AEs occurred in 55% of patients receiving combination nivolumab/ipilimumab compared with 16.3% in patients treated with nivolumab alone, and 27.3% of patients treated with ipilimumab. High-grade AEs associated with the combination included diarrhea (9.3%), increased lipase (8.6%), increased ALT (8.3%), and colitis (7.7%). Similarly, in the Checkmate-069 study, the combination caused a higher rate of serious diarrhea (13% and 2.6%), colitis (10% and 1.6%) and pyrexia (10% and 0.6%) compared with nivolumab monotherapy (TABLE 2).14
TABLE 2. Adverse Events With Frontline Combination Regimens
All-Grade
Grade 3/4
COMBI-v (dabrafenib/trametinib)
98%
49%
COMBI-d (dabrafenib/trametinib)
87%
32%
coBRIM (vemurafenib/cobimetinib)
96%
65%
CheckMate-069 (ipilimumab/nivolumab)
91%
54%
CheckMate-067 (ipilimumab/nivolumab)
96%
55%
According to Jeffery S. Weber, MD, PhD, with the NYU Langone Medical Center, New York, “the toxicity is significant. Much of it is biochemical, such as grade 3 hyperamylasemia with no symptoms.” However, “A 14% rate of grade 3/4 colitis and diarrhea is a big problem, particularly when you add the diarrhea and the colitis together, which in the toxicity ratings are often separate.”
REFERENCES
- Fedorenko IV, Gibney GT, Sondak VK, Smalley KS. Beyond BRAF: where next for melanoma therapy?Br J Cancer.2015;112:217-226.
- Hugo W, Shi H, Sun L, et al. Non-genomic and Immune Evolution of Melanoma Acquiring MAPKi Resistance.Cell.2015;162:1271-1285.
- Sanlorenzo M, Choudhry A, Vujic I, et al. Comparative profile of cutaneous adverse events: BRAF/MEK inhibitor combination therapy versus BRAF monotherapy in melanoma.J Am Acad Dermatol.2014;71:1102-1109.e1.
- Robert C, Karaszewska B, Schachter J, et al. Two year estimate of overall survival in COMBI-v, a randomized, open-label, phase III study comparing the combination of dabrafenib (D) and trametinib (T) with vemurafenib (Vem) as first-line therapy in patients (pts) with unresectable or metastatic BRAF V600E/K mutation-positive cutaneous melanoma. Presented at: 2015 European Cancer Congress; September 25-29; Vienna, Austria Abstract 3301.
- Long GV, Stroyakovskiy D, Gogas H, et al. Overall survival in COMBI-d, a randomized, double-blinded, phase III study comparing the combination of dabrafenib and trametinib with dabrafenib and placebo as first-line therapy in patients (pts) with unresectable or metastatic BRAF V600E/K mutation-positive cutaneous melanoma.J Clin Oncol.2015;33:(suppl; abstr 102).
- Long GV, Stroyakovskiy D, Gogas H, et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-blind, phase 3 randomised controlled trial.Lancet.2015;386:444-451.
- Robert C, Karaszewska B, Schachter J, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib.N Engl J Med.2015;372:30-39.
- Grob JJ, Amonkar MM, Karaszewska B, et al. Comparison of dabrafenib and trametinib combination therapy with vemurafenib monotherapy on health-related quality of life in patients with unresectable or metastatic cutaneous BRAF Val600-mutation-positive melanoma (COMBI-v): results of a phase 3, open-label, randomised trial.Lancet Oncol.2015;16:1389-1398.
- Larkin J, Ascierto PA, Dreno B, et al. Combined vemurafenib and cobimetinib in BRAF-mutated melanoma.N Engl J Med.2014;371:1867-1876.
- Larkin J, Yan Y, McArthur GA, et al. Update of progression-free survival (PFS) and correlative biomarker analysis from coBRIM: Phase III study of cobimetinib (cobi) plus vemurafenib (vem) in advanced BRAF-mutated melanoma.J Clin Oncol.2015;33:(suppl; abstr 9006).
- Atkinson V, Larkin J, McArthur GA, et al. Improved overall survival with cobimetinib (COBI) and vemurafenib (VEM) in advanced BRAFV600-mutated melanoma and biomarker correlates of efficacy. Abstract presented at the 12th International Congress of the Society for Melanoma Research in San Francisco, California, 21 November 2015.
- Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma.N Engl J Med.2015;373:23-34.
- Postow MA, Chesney J, Pavlick AC, et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma.N Engl J Med.2015;372:2006-2017.
- Postow MA, Chesney J, Pavlick AC, et al. Initial report of overall survival rates from a randomized phase II trial evaluating the combination of nivolumab (NIVO) and ipilimumab (IPI) in patients with advanced melanoma (MEL). Presented at: AACR 2016, New Orleans; April 16-20, 2016.
However, because of the a “very steep and immediate response” associated with combination immunotherapy with nivolumab and ipilimumab, Weber considers this regimen “the treatment of choice for anyone with rapidly progressive, high-LDH, aggressive, symptomatic disease.”











Savona Discusses First-Line JAK Inhibition for Patients With Myelofibrosis at Risk of Anemia
April 17th 2024During a Case-Based Roundtable® event, Michael Savona, MD, and participants discussed the case of a patient with myelofibrosis and moderate anemia receiving JAK inhibitor therapy.
Read More

