Panel Addresses Integration of PARP Inhibitors Into Breast Cancer Space
At the <em>36th Annual </em>Miami Breast Cancer Conference<sup>®</sup>, a panel of experts discussed the use of 2 FDA-approved PARP inhibitors for patients with HER2-negative advanced or metastatic breast cancer whose tumors are positive for germline <em>BRCA1/2 </em>mutations.


Mark E. Robson, MD

Mark E. Robson, MD
PARP inhibitors have proven to be a significant advance in the treatment landscape of patients with advanced breast cancer who have germlineBRCA1/2mutations. However, these agents still need to be optimized in this setting, leading experts say.
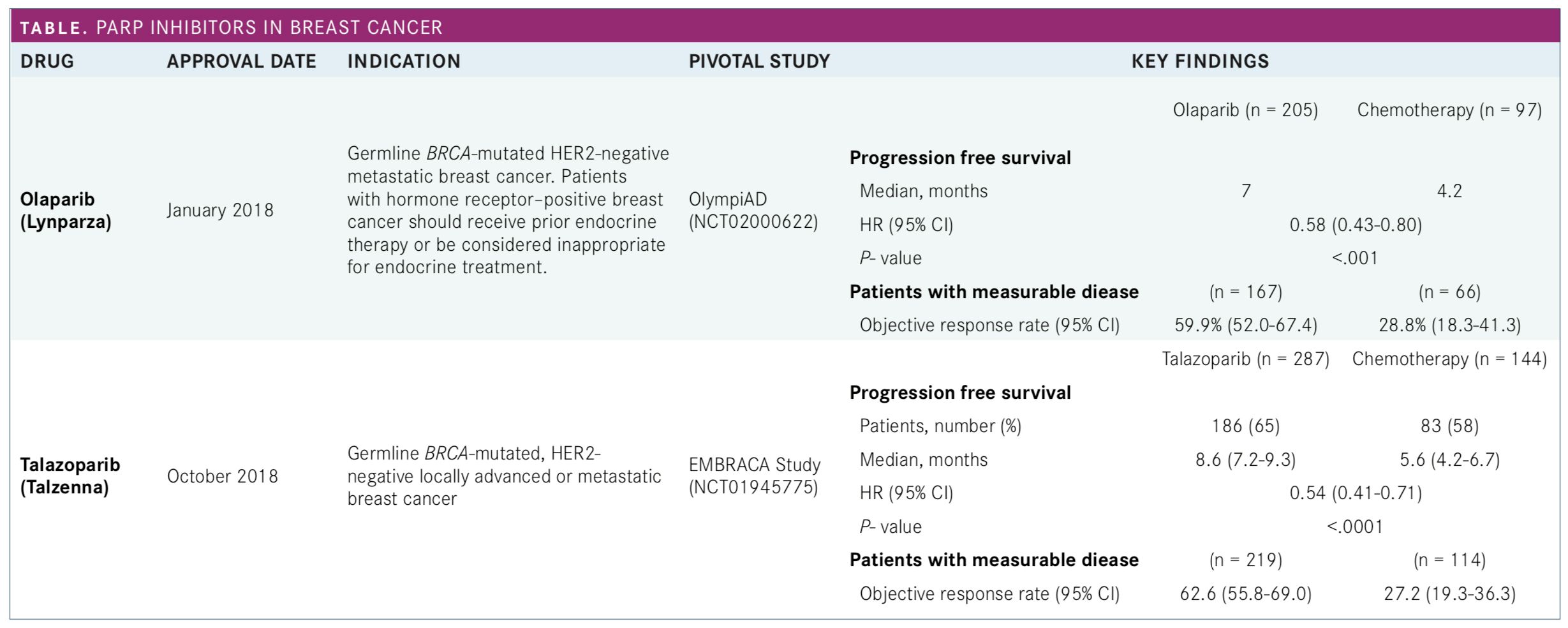
At the36th AnnualMiami Breast Cancer Conference®, a panel of experts discussed the use of 2 FDA-approved PARP inhibitors for patients with HER2-negative advanced or metastatic breast cancer whose tumors are positive for germlineBRCA1/2mutations (Table).
A similar improvement in progression-free survival (PFS) of approximately 3 months were demonstrated in pivotal trials compared to standard chemotherapy. Although those findings led to the approval of both agents, panelists said that the goal is to improve these outcomes further.
“There’s a whole host of different approaches that can be taken to try to extend the benefits of the very promising early findings,” said Mark E. Robson, MD, who chaired the discussion. “We do have to be cautious in our optimism but I would point out that if you go back and look at the original [trastuzumab] Herceptin trial, the PFS advantage was only about 4 or 5 months, so I think it’s just a question of trying to find how well we can make this work and can we extend the benefits.”
Robson, who was the lead investigator on the pivotal olaparib study, is chief of the Breast Medicine Service at Memorial Sloan Kettering Cancer Center and a professor of medicine at Weill Cornell Medical College, both in New York City.
He said that the next steps in the research include testing combinations of PARP inhibitors with therapies that targetPIK3CAmutations, VEGF, DNA replication stress (ATM and ATR inhibitors), and BET and TOPO1 inhibitors. Additionally, PARP inhibitors will be evaluated in combination with immunotherapy agents.
However, combining PARP inhibition with chemotherapy is not a promising strategy, Robson said. “It’s extremely challenging, largely because of overlapping myelosuppression,” he said. “It’s very difficult to get full-dose PARP inhibition and full-dose myelosuppressive therapy despite the fact that there are potentially advantages to doing that.”
Table. PARP Inhibitors in Breast Cancer


Table. PARP Inhibitors in Breast Cancer
Key Findings in Pivotal Trials
Other areas to be explored include testing PARP inhibitors in the neoadjuvant and adjuvant settings, trying the agents against other genes and somatic mutations, and learning from PARP research in other cancers, particularly emerging information in pancreas and prostate cancers.The olaparib approval was based on the results of the phase III OlympiAD study, in which patients were randomized 2:1 to receive olaparib at 300 mg twice daily or standard therapy with single-agent chemotherapy of the physician’s choice (capecitabine, eribulin, or vinorelbine in 21-day cycles). Progression-free survival (PFS), the primary endpoint, was 7.0 months with olaparib versus 4.2 months with standard therapy. That translated into a hazard ratio (HR) for disease progression or death favoring olaparib of 0.58 (95% CI, 0.43-0.80;P<.001).1
In the phase III EMBRACA trial, patients were randomized 2:1 to receive talazoparib at 1 mg once daily or physician’s choice of the same single-agent chemotherapy agents offered in OlympiAD. The median PFS was 8.6 months with talazoparib versus 5.6 months with chemotherapy. The hazard ratio for disease progression or death favoring talazoparib was 0.54 (95% CI, 0.41-0.71;P<.001).2
Notably, both drugs performed well when health-related quality of life was assessed using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (QLQ-C30). The median time to a clinically meaningful decrease in QLQ-C30 score (≥10 points) was not reached among patients who received olaparib compared with 15.3 months for those who had chemotherapy (HR, 0.44; 95% CI, 0.25-0.77;P= .004).1
For talazoparib, investigators reported a statistically significant delay in the time to clinically meaningful deterioration on the QLQ-C30. The median time to deterioration was 24.3 months with talazoparib (95% CI, 13.8-not reached) compared with 6.3 months (95% CI, 4.9-12.2) for with chemotherapy (HR, 0.38; 95% CI, 0.26-0.55;P<.0001).3
Panel members said those findings are further evidence that the drugs are improving the lives of patients.
Neoadjuvant Study
In terms of adverse events (AEs), panel members said anemia is an important consideration. The most prevalent grade 3/4 AEs with olaparib in the OlympiAD study included anemia (16.3%), neutropenia (9.3%), and fatigue (2.9%). In the EMBRACA study, the most prevalent grade 3/4 AEs were anemia (39.2%), neutropenia (20.1%), and thrombocytopenia (14.7%)Robson said he generally believes that early treatment improves outcomes and pointed to findings from a small study conducted by panel member Jennifer K. Litton, MD, as an indication that neoadjuvant PARP inhibition could be effective. Litton, the lead investigator on the EMBRACA study, is an associate professor in the Department of Breast Medical Oncology at The University of Texas MD Anderson Cancer Center in Texas.
In the small neoadjuvant study, talazoparib was administered at 1 mg daily to patients with germlineBRCA-positive stage I to III breast cancer with tumors >1 cm. To be eligible, patients could not have received prior therapy for invasive breast cancer or have HER2-positive disease. Talazoparib therapy was followed by surgery and then systemic physician’s choice therapy. The primary endpoint was pathological complete response (pCR), defined as ypT0/is ypN0).4
Of the 20 patients who participated in the study, 15 had triple-negative breast cancer (TNBC) and 5 were hormone receptorpositive. Of the patients for whom results were available, 10 of 19 achieved pCR (53%) with residual cancer burden (RCB) of 0, and 12 of 19 (63%) had an RCB of 0 or 1.
The study marked the first time a single targeted therapy demonstrated pCR activity in patients withBRCA-positive breast cancer, Litton said in presenting the findings at the 2018 American Society of Clinical Oncology Annual Meeting. The positive results have prompted the initiation of the larger NEOTALA study in patients with TNBC.
“This has now expanded to a nationwide study so we can see the effect on a larger patient size,” Litton said during the panel discussion. “I’m hopeful that we’ll see the same responses, if not better.”
References:
- Robson M, Im SA, Senkus E, et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation.N Engl J Med. 2017 Aug 10;377(6):523-533. doi: 10.1056/NEJMoa1706450.
- Litton JK, Rugo HS, Etti J, et al; Talazoparib in patients with advanced breast cancer and a germline BRCA mutation.N Engl J Med. 2018;379(8):753-763. doi: 10.1056/NEJMoa1802905.
- Ettl J, Quek RGW, Lee KH, et al. Quality of life with talazoparib versus physician's choice of chemotherapy in patients with advanced breast cancer and germline BRCA1/2 mutation: patient-reported outcomes from the EMBRACA phase III trial.Ann Oncol. 2018;29(9):1939-1947.
- Litton JK, Scoggins M, Hess KR, et al. Neoadjuvant talazoparib (TALA) for operable breast cancer patients with a BRCA mutation (BRCA+).J Clin Oncol. 2018;36(suppl; abstr 508). meetinglibrary.asco.org/record/160762/abstract.






Breast Cancer Leans into the Decade of Antibody-Drug Conjugates, Experts Discuss
September 25th 2020In season 1, episode 3 of Targeted Talks, the importance of precision medicine in breast cancer, and how that vitally differs in community oncology compared with academic settings, is the topic of discussion.
Listen

Experts Warn of Radiation Overtreatment in Older Women With Early-Stage Breast Cancer
March 20th 2024Studies have found that omitting radiation therapy after breast-conserving surgery and/or omitting axillary surgery in women age 70 years or older does not affect their survival when taking endocrine therapy.
Read More

