Unprecedented Response Rates Seen With Ipilimumab Plus Nivolumab in Melanoma
Results from the phase II, double-blind CheckMate-069 clinical trial showed unprecedented response rates with ipilimumab combined with nivolumab in previously treated patients with metastatic melanoma.


F. Stephen Hodi, MD

F. Stephen Hodi, MD
Background
Results from the phase II, double-blind CheckMate-069 clinical trial1presented April 20, 2015 at the Annual Meeting of the American Association for Cancer Research showed unprecedented response rates with ipilimumab (Yervoy) combined with nivolumab (Opdivo) in previously treated patients with metastatic melanoma. Preclinical studies supported this possibility and other immunotherapy combination studies in melanoma are currently under way.In 2013 Wolchok et al published findings from a phase I trial2 of ipilimumab (IPI) and nivolumab (NIVO) in combination in previously treated patients with metastatic melanoma.
“Preclinical studies suggested that this combination therapy would have better outcomes than those elicited by their individual or sequential administration,” said F. Stephen Hodi, MD, director of the Melanoma Treatment Center and director of the Center for Immuno-Oncology at the Dana-Farber Cancer Institute, Boston, MA.3
The results of the phase I clinical trial showed an objective response rate (ORR) of 40% with evidence of clinical activity in 65% of patients. Most impressive, was an up to 80% reduction in tumor volume at the maximum tolerated dose.2
CheckMate-069
“It was apparent following that trial that the combination should be tested as a first-line therapy for metastatic melanoma,” said Jedd D. Wolchok, MD, PhD, chief, melanoma and immunotherapeutics service, Lloyd J. Old Chair for Clinical Investigation, Memorial Sloan Kettering Cancer Center, New York, NY. “Rationally combined immunotherapies hold great promise for cancer treatment as long as their side effects can be managed.”3This phase II trial (CheckMate-069)3was double blind and patients were randomized 2:1 to receive and 3 mg/kg IPI and NIVO at 1 mg/kg (n = 95) or placebo (n = 47) once every 3 weeks for 4 doses. IPI was then discontinued and patients received NIVO at the same dose or placebo, until disease progression or unacceptable toxicity.
Inclusion criteria required patients were treatment naïve with stage III or IV melanoma, and known BRAF V600 status, with a tissue sample for PD-L1 assessment. Exclusion criteria included active brain metastases, uveal melanoma, and serious autoimmune disease.
The primary endpoint was the ORR in patients with BRAF V600 wild-type (WT) tumors. Secondary endpoints included progression-free survival (PFS) in patients with BRAF wild-type tumors, ORR and PFS in patients withBRAF V600-mutationpositive tumors, and safety.
Response Rates: BRAF WT
A total of 142 patients were enrolled, the majority of patients were male, and 87% of patients had stage IV disease.BRAF V600-mutationpositive tumors were found in 23% of patients. Thus 109 patients had BRAF WT tumors and 33 hadBRAF V600-mutationpositive tumors.“Patients who received the combination had significantly higher response rates, particularly in the wild-type population,” Hodi said.4
Figure 1: Primary endpoint.


Figure 1: Primary endpoint.
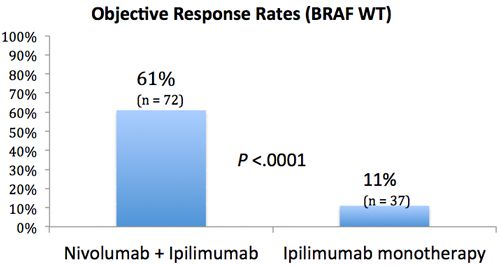
There was a statistically significant difference in ORRs between the two groups (Figure) with a greater number of responses in the NIVO + IPI group (44/72) than in the IPI monotherapy group (4/37). Considering NIVO + IPI versus IPI monotherapy, complete responses (CR) were achieved in 22% of patients versus none, respectively. Partial responses (PRs) were noted in 39% versus 11%, stable disease (SD) in 12% versus 35%, and progressive disease (PD) in 14% versus 41% of patients, respectively.
An ongoing response was achieved in 36/44 (82%) patients who had an objective response in the NIVO + IPI group versus 3 of 4 patients (75%) in the IPI monotherapy group. Median duration of response was not reached by either group and time to a response was not significantly different between the groups.
Median PFS was not reached in the combination group, but was 4.4 months in the monotherapy group (HR = 0.40; 95% CI, 0.23-0.68;P<.001)
Tumor volumes as assessed by investigators, were reduced by a median of 68.1% in the NIVO + IPI group versus an increase of 5.5 % in the IPI monotherapy group.
Data showed that the impact of combination therapy on ORR was independent of tumor PD-L1 status. The ORR was 58% (95% CI, 37 to 78) in patients with PD-L1positive tumors versus 55% (95% CI, 41to 69) in patients with PD-L1–negative tumors. For patients in the IPI monotherapy group, ORR was numerically higher for patients with PD-L1 positive tumors versus PD-L1 negative tumors, 18% versus 4% (95% CI, 2 to 52, and 95% CI, 0 to 19, respectively).
Response Rates: BRAF V600 Mutation
Hodi and colleagues stated that, “These data suggest that PD-L1 should not be used to select patients to receive combination treatment.” Contrasting these results with previous studies showed an association between higher response rates with NIVO monotherapy and positive PD-L1 expression.1Patients who had the BRAF V600 mutation and received NIVO + IPI had an ORR of 52% (12/23) versus 10% (1/10) in the IPI monotherapy group. Considering the combination group versus the monotherapy group, CR was 22% versus 0%, PR was 30% versus 10%, SD was 13% versus 10% and PD was 22% versus 70%.
Median PFS was 8.5 months in the combination therapy group and 2.7 months in the monotherapy group (HR = 0.38; 95% CI, 0.15-1.00).
Side Effect Profile
“These results are consistent with the results of a previous phase I trial, and suggest that the presence of theBRAF V600mutation does not influence the efficacy of checkpoint blockade,” Hodi et al stated in theNEJMarticle.1Grade 3/4 side effects related to drug occurred in 54% of patients in the combination group and in 24% in the IPI monotherapy group.
Table: Most Common Grade 3/4 Adverse Events
Adverse Event
NIVO + IPI (n = 94)
IPI Monotherapy (n = 46)
Colitis
17%
7%
Diarrhea
11%
11%
Elevated alanine aminotransferase
11%
“In general, and as might be expected, side effects were more prevalent in patients who received the combination therapy,” said Hodi. “This is something that will have to be studied further.”3The most common grade 3/4 adverse events cited by the study authors are shown in the Table.Adverse events attributed to an immune cause were experienced by more patients in the combination group than the IPI monotherapy group, and consequently patient use of immunosuppressive medications to ameliorate these events were greater in the combination arm (89% vs 59%). The majority of treated immune-related events were resolved or symptoms were reverted to baseline levels.
The majority of discontinuations in the combination group (45%) were because of drug-related adverse events, but Hodi explained, “Even in those patients that required stopping the drug due to toxicities, 68% of those patients continued to have either partial responses or complete responses to therapy.”4
Disease progression accounted for the majority of discontinuations (37%) in the IPI monotherapy arm. Of the total number of deaths in the study, the majority were due to progressive disease (higher in the IPI monotherapy group, 37% vs 27%). Three deaths were attributed to combination therapy.
Future Prospects
“These data are unprecedented in advanced melanoma, showing efficacy results that have not previously been observed with Immuno-Oncology agents,” said Hodi in a statement. “With the nivolumab plus ipilimumab regimen, we observed much higher response rates, which were sustained, as well as significant reduction in tumor burden than with ipilimumab. These responses seen in CheckMate-069 demonstrate the potential of this regimen in patients with metastatic melanoma.”5The clinical trial program for this combination continues. With an estimated primary completion date of September 2016, the phase III CheckMate 067 (NCT01844505) double-blind study has recruited previously untreated patients with unresectable or metastatic melanoma, randomized to NIVO monotherapy or NIVO + IPI versus IPI monotherapy. The primary endpoints are OS and PFS.
Clinical Pearls
- Preclinical data suggest combining NIVO and IPI would yield better outcomes than when used as single agents.
- A phase I study of the combination in previously treated patients with metastatic melanoma yielded objective response in 53% of patients and tumor reduction of ≥80% at the highest tolerated dose.
- CheckMate 069 randomized 142 treatment-naïve patients with metastatic melanoma to combination therapy of NIVO with IPI, or IPI and placebo once every 3 weeks for 4 doses, and then NIVO or placebo every 2 weeks until disease progression or unacceptable toxicity.
- Patients with BRAF WT tumors receiving NIVO plus IPI experienced a 61% ORR, with a 22% complete response rate.
- Patients with BRAF WT tumors who only received IPI had an ORR of 11% and no complete responses.
- Patients with BRAF V600 mutations experienced similar results as patients with BRAF WT tumors.
- Median PFS was not reached in the NIVO + IPI group and was 4.4 months in the IPI monotherapy group.
- Grade 3/4 drug-related adverse events were experienced by 54% of patients receiving NIVO + IPI versus 24% receiving IPI monotherapy.
- The data reveal the potential of immunotherapy combinations in the management of cancer
Ipilimumab is also being investigated in combination with several agents in melanoma, notably, with talimogene laherparepvec. A phase Ib/II trial is currently recruiting patients with unresectable stage III/IV melanoma to assess the safety of talimogene laherparepvec with IPI versus IPI monotherapy (NCT01740297). The estimated primary completion date is May 2016.
References
- Postow MA, Chesney J, Pavlick AC et al. Nivolumab and Ipilimumab versus Ipilimumab in Untreated Melanoma.N Engl J Med. 2015 E. pub April 20 DOI: 10.1056/NEJMoa141428.
- Wolchok JD, Kluger H, Callahan MK, et al. Nivolumab plus ipilimumab in advanced melanoma.N Engl J Med.2013;369:122-133.
- Immunotherapy combination promising for untreated patients with advanced melanoma. http://www.newswise.com/articles/immunotherapy-combination-promising-for-untreated-patients-with-advanced-melanoma. Published April 20, 2015. Accessed April 20, 2015.
- Dr. Hodi on nivolumab in combination with ipilimumab for advanced melanoma. http://www.onclive.com/conference-coverage/aacr-2015/Dr-Hodi-on-Nivolumab-in-Combination-With-Ipilimumab-for-Advanced-Melanoma. Published April 20, 2015. Accessed April 20, 2015.
- Adding nivolumab to frontline ipilimumab improves PFS by 60% in melanoma. http://www.onclive.com/conference-coverage/aacr-2015/Adding-Nivolumab-to-Frontline-Ipilimumab-Improves-PFS-by-60-in-Melanoma. Published April 20, 2015. Accessed April 20, 2015.
<<<

















Savona Discusses First-Line JAK Inhibition for Patients With Myelofibrosis at Risk of Anemia
April 17th 2024During a Case-Based Roundtable® event, Michael Savona, MD, and participants discussed the case of a patient with myelofibrosis and moderate anemia receiving JAK inhibitor therapy.
Read More

