New Targeted Therapy in Acute Lymphocytic Leukemia: A Review of Blinatumomab in Relapsed/Refractory Acute Lymphocytic Leukemia
Acute lymphoblastic leukemia (ALL) is a relatively rare malignancy in adults, with an estimated 6250 new cases and 1450 deaths expected in the United States in 2015. Although most patients achieve complete remission with conventional combination chemotherapy regimens, at least two-thirds of high-risk patients relapse.2 While overall survival for children has significantly improved in the last 30 years, newly diagnosed adults continue to have a poor 5-year OS rate, approximating 35%, depending on age and risk factors.


soft tissue sarcoma

Cindy Herrera, PharmD, BCPS
Introduction
Acute lymphoblastic leukemia (ALL) is a heterogeneous hematologic malignancy characterized by the proliferation of immature lymphoid cells in the bone marrow. ALL is a relatively rare malignancy in adults, with an estimated 6250 new cases and 1450 deaths expected in the United States in 2015.1Although most patients (>80%) achieve complete remission (CR) with conventional combination chemotherapy regimens, at least two-thirds of high-risk patients relapse.2While overall survival (OS) for children has significantly improved in the last 30 years, newly diagnosed adults continue to have a poor 5-year OS rate, approximating 35%, depending on age and risk factors.3,4
Outcomes for relapsed/refractory patients remain worse: Only ~30%-45% of patients achieve a second CR, with a 5-year OS of 7%-10%.2,3,5Salvage regimens consist mainly of high-dose combination chemotherapy, including augmented hyper-fractionated cyclophosphamide, vincristine, doxorubicin, dexamethasone, and PEG-asparaginase (hyper-CVAD), alternating with methotrexate and cytarabine, and clofarabine-, cytarabine-, or alkylator-combination regimens, and liposomal vincristine.6,7Hematopoietic stem cell transplantation (HSCT) remains the only curative option for adult patients with ALL.
Blinatumomab (Blincyto, MT103, Amgen Inc, Thousand Oaks, CA) is the first-in-class bispecific T-cell engager (BiTE) antibody approved by the US Food and Drug Administration (FDA). Blinatumomab’s mechanism allows it to physically link T cells to malignant B cells by simultaneously binding CD3 on cytotoxic T cells and CD19 on B cells. It received breakthrough therapy designation in December 2014 for the treatment of Philadelphia chromosome-negative (Ph-) relapsed or refractory precursor B-cell ALL (B-ALL).8The National Comprehensive Cancer Network (NCCN) lists blinatumomab as a category 2A recommendation for Ph- relapsed/refractory B-ALL.7. The purpose of this article is to review the mechanism of action, pharmacokinetics/pharmacodynamics, clinical efficacy, adverse effects (AEs), dosage, administration, and future directions for blinatumomab.


melanoma

Hillary Prescott, PharmD
Data Sources
A PubMed search of the key termsblinatumomabandMT103was conducted in April and May 2015. Other information was obtained from the product labeling, ClinicalTrials.gov, and the FDA approval letters, reviews, accepted abstracts, and related documents.
Mechanism of Action
Blinatumomab is a BiTE®antibody engineered to incorporate a linker sequence that allows it to be reduced to two variable binding domains on a single polypeptide chain, essentially combining two single-chain antibodies with different binding specificity in tandem. This functionally allows for cell lysis independent of the major histocompatibility complex (MHC)-1-peptide-T cell receptor (TCR) complex.9,10
Cytotoxic T cells are the most potent and effective killer cells. They lack Fcγ receptors and are therefore unable to participate in the regular antibody-dependent cellular cytotoxicity (ADCC) that relies on the binding of Fcγ receptors on cytolytic immune cells to the Fc region on antibodies. Blinatumomab is the first type of antibody therapy that is able to overcome this obstacle in activating the immune T-cell response.
T cells are effective killer cells because of their mechanism of cell lysis; they contain vesicles that harbor pore-forming perforins and proteases (granzymes) that are subsequently delivered onto the target cell. This is only possible once the cytotoxic T cell is bound to its target through the MHC-1-TCR complex. Blinatumomab engages T cells by forming a cytolytic synapse between the CD3-bound T cell and the CD19-bound B cell. The CD3 binding on blinatumomab to cytotoxic T cells activates the T cells, circumventing the MHC-1-TCR binding, which is its typical mechanism of activation. Blinatumomab does not remain attached to the target cell during its lysis and therefore is able to be recycled and subsequently activate other T cells. The CD3 binding region on blinatumomab allows monovalent binding to all T cells with low affinity, triggering T-cell signaling only when presented with multivalent binding to target cells, therefore redirecting tumor cell lysis only when concomitantly bound to a CD19+ B cell.10Once engaged, blinatumomab activates T cells and then releases cytokines (ie, interleukin 2 [IL-2], IL-6, IL-10, interferon gamma [INF-γ]), induces B-cell apoptosis, and produces a polyclonal expansion of memory T cells.11,12An advantage of targeting CD19 is its expression on most B-lineage malignancies, while lacking expression on hematopoietic stem cells and plasma cells. Its expression by early pre-B cells through mature B- cell development has shown to involve the PI3 kinase pathway, therefore magnifying B-cell activation and survival signaling.13,14


melanoma

Daniel Wojenski, PharmD, BCPS, BCOP
Pharmacokinetics and Pharmacodynamics
In the adult dose-finding studies, there was no clinically meaningful effect of size or weight on blinatumomab clearance (age 18-80 years; body weight 44 kg to 134 kg; body surface area [BSA] 1.39-2.57 m2). Hence, flat dosing for blinatumomab can be used. The dose of 9 µg/day was based on the initial 5 µg/m2/day dose and the 28 µg/day dose was based on 15 µg/m2/day in an average-sized adult (BSA 1.8 m2).15Initially, phase I studies used short-term infusion dosing in patients with non-Hodgkin lymphoma (NHL) and blinatumomab was given once, twice, or three times a week as a 2-hour or 4-hour IV infusion. The phase I studies that used short-term infusions were terminated early because of lack of efficacy likely related to the lack of sustained reduction of peripheral CD19+ cells, the short serum half-life of blinatumomab, and its mechanism of action that focuses on continued B-cell depletion and prolonged T-cell activation.16Blinatumomab demonstrated linear pharmacokinetics in terms of dose proportionality and time-dependent clearance. The mean half-life was ~2 hours, which requires continuous infusion dosing to obtain adequate serum concentrations. The mean volume of distribution in adult patients was estimated at ~5 L.15
Only 0.2% of unchanged blinatumomab was shown to be eliminated in the urine. Additionally, clearance among patients with mild to moderate renal dysfunction was similar to that in patients with normal renal function (1.6 L/hr to 3.3 L/hr); therefore, patients with mild to moderate renal dysfunctin do not require a dose adjustment. In clinical trials, patients with mild to moderate renal dysfunction experienced a higher incidence of grade 3 and 4 toxicities, although this was confounded by age, given that elderly patients could have an increased risk of AEs and renal dysfunction. It is worth noting that patients with severe renal impairment (creatinine clearance[CrCL] <30 mL/min) were excluded from the trials, so that no dosing recommendations can be made for this population.15,17
There was no association between baseline transaminase levels and the clearance of blinatumomab. While the metabolic pathway has not been elucidated, it is expected to follow normal protein catabolic pathways.17
In terms of blinatumomab’s pharmacodynamic properties, complete B-cell depletion was dose dependent and achieved within 48 hours at doses ≥5 µg/m2/day in patients with NHL.19Cytokines (IL-6, IL-10, INF-γ) were elevated in more than 50% of patients with relapsed/refractory ALL on days 1-2 of cycle 1, and less in later cycles.20
Clinical Trials
For the purpose of this review, we will highlight the studies that gained blinatumomab approval for Ph- precursor B-ALL, including the dose-finding phase II study that supports the approved dosing.

Phase II in Ph- relapsed/Refractory B-ALL
A small phase II study by Topp et al evaluated three sequential blinatumomab dosing cohorts in 36 patients with relapsed/refractory B-ALL.21Patients had ≥5% leukemic bone marrow blasts, an Eastern Cooperative Oncology Group (ECOG) performance status of ≤2, and had Ph- disease or Philadelphia chromosome-positive (Ph+) disease unable to be treated with tyrosine kinase inhibitors (TKIs). Blinatumomab was given as an intravenous continuous infusion (IVCI) for 4 weeks every 6 weeks. During the first cohort of the dosing-finding run-in phase, patients (n = 7) received blinatumomab 15 µcg/m2/day IVCI on days 1-28 (cohort 1). After one patient experienced grade 4 cytokine-release syndrome (CRS), a dose-step approach was implemented and a dexamethasone prephase (up to 24 mg/m2per day for ≤5 days and/or cyclophosphamide 200 mg/m2for ≤4 days) was permitted. Patients in cohort 2a (n = 5) received a starting dose of 5 µg/m2/day IVCI on days 1-7, then increased to 15 µg/m2/day IVCI for days 8-28. Finally, patients in cohort 2b (n = 6) received 5 µg/m2/day IVCI on days 1-7, then 15 µg/m2/day IVCI on days 8-14, followed by 30 µg/m2/day IVCI on days 15-28. Cohort 1 had the highest rates of AEs overall while cohort 2a, had the lowest rates of AEs and, therefore, was the treatment approach used to treat 18 patients in the extension stage. Among all patients, 69% achieved a CR or CR with partial hematologic recovery (CRh) of peripheral blood counts (n = 15 CR, n = 10 CRh), with the lowest proportion of CR/CRh in those who had relapsed after HSCT. One of the two patients with Ph+ B-ALL achieved CR/CRh. Among the 25 responders, 88% (n = 22) achieved a minimal residual disease (MRD) response, defined as a decrease of MRD to <10-4blasts by polymerase chain reaction (PCR). Median relapse-free survival (RFS) was 7.6 months and median OS (mOS) was 9.8 months (mOS if CR = 13.2 months; CRh = 8.3 months), and of the 25 responders, 52% (n = 13) proceeded to HSCT.
The phase II confirmatory study that led to blinatumomab’s accelerated approval was a multicenter, single-arm, open-label study by Topp et al that enrolled 189 patients with Ph-, relapsed/refractory precursor B-ALL.22Patients were either primary refractory after induction, relapsed within 12 months of first remission or after having received allogeneic (allo-) HSCT, or failed or relapsed after at least first salvage therapy. Patients with central nervous system or testicular involvement, Ph+ B-ALL, ECOG performance status >2, acute or grade 2-4 chronic graft-versus-host-disease (GVHD), autoimmune disease, auto-HSCT within 6 weeks or allo-HSCT within 3 months of starting blinatumomab, and hepatic or renal insufficiency were excluded. Chemotherapy, radiation, and systemic treatment of GVHD were not allowed within 2 weeks of starting blinatumomab.
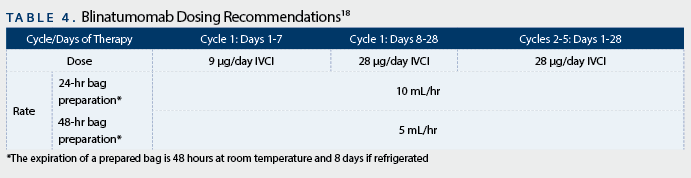
Blinatumomab was given as an IVCI at a target dose of 28 µg/day (9 µg/day on days 1-7, followed by 28 µg/day on days 8-28 in cycle 1; 28 µg/day on days 1-28 in cycles 2-5). This was given every 6 weeks for up to 5 cycles. Patients were premedicated with dexamethasone 20 mg within 1 hour of starting treatment in each cycle and before the dose step in cycle one. Patients with bone marrow blasts >50%, peripheral blood blasts ≥15,000 cells/mcL, or elevated lactate dehydrogenase (LDH) levels were treated with a dexamethasone prephase of 10-24 mg/m2per day for up to 5 days because of the high risk for CRS. The primary endpoint was CR + CRh within the first 2 cycles.
Of the 189 patients, 39% had failed ≥2 prior salvage regimens, 34% relapsed after allo-HSCT, and 69% had bone marrow blasts >50%. Patients received blinatumomab for a median of 42.2 days, and 51% of patients received the dexamethasone prephase treatment. Forty-three percent of patients achieved CR/CRh (n = 81/189; 33% CR, 10% CRh) within the first 2 cycles, with most (79%) of CR/CRh achieved in cycle 1. Patients with a lower percentage of bone marrow blasts (<50%) at presentation were more likely to achieve CR/CRh compared with those with ≥50% bone marrow blast (73% vs 29%); however, response was seen across all subgroups in respect to age and prior lines of therapy, including HSCT. Median RFS was 5.9 months for the 82 patients in CR/CRh and median OS was 6.1 months for all 189 patients. Of the patients who achieved CR/CRh, 40% proceeded to allo-HSCT after receiving at least 2 cycles of blinatumomab and had a 100-day mortality rate of 11%. Of the 73 patients evaluable for MRD, 82% (n = 60) achieved MRD negativity. Although RFS and OS were relatively short, median RFS was longer for patients with MRD-negativity in CR/CRh compared with patients without MRD response (6.9 vs 2.3 months), as was OS (11.5 vs 6.7 months). It is worth noting that response rates were achieved despite the patient population having several negative prognostic factors, including high tumor burden and failure of multiple lines of salvage therapy, which typically correlate with low response rates to therapy.
Adverse Effects
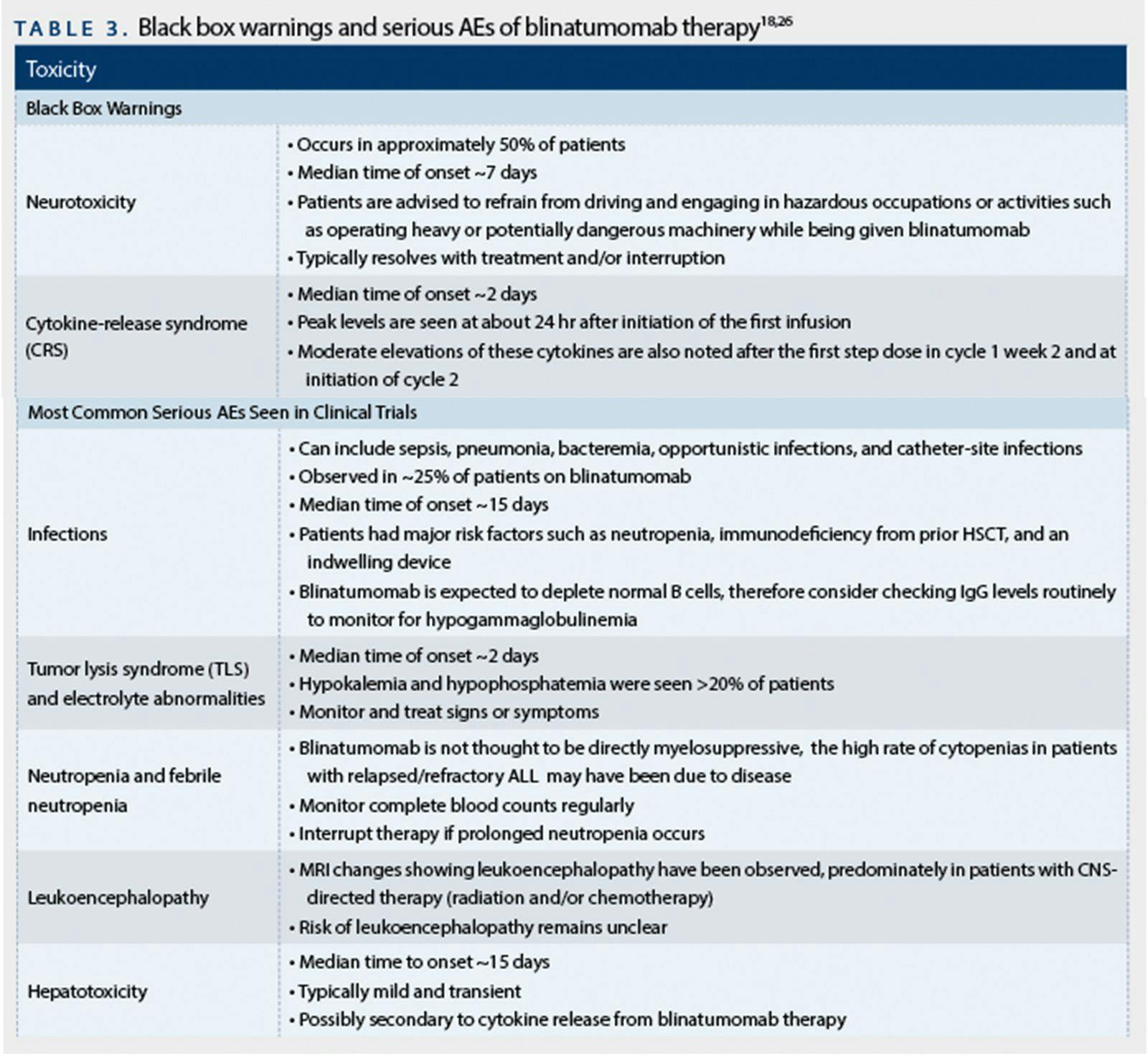
In the confirmatory Topp et alstudy,2299% of patients experienced at least one AE of any grade, most commonly pyrexia (60%), headaches (34%), febrile neutropenia (28%), peripheral edema (26%), nausea (26%), hypokalemia (24%), constipation (21%), and anemia (20%). The most common grade 3 or 4 AEs were hematologic in nature: febrile neutropenia (25%), neutropenia (16%), and anemia (14%). Twelve percent of patients (n = 23) had fatal AEs, predominately infection-related (74%), which is not uncommon in this patient population. Three patients experienced grade 3 CRS, and 52% (n =9 8) of patients had neurologic events (11% grade 3-4).
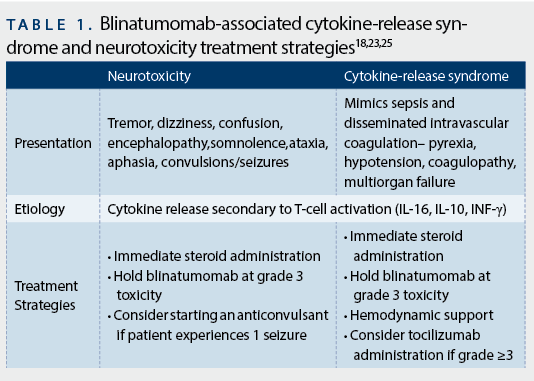
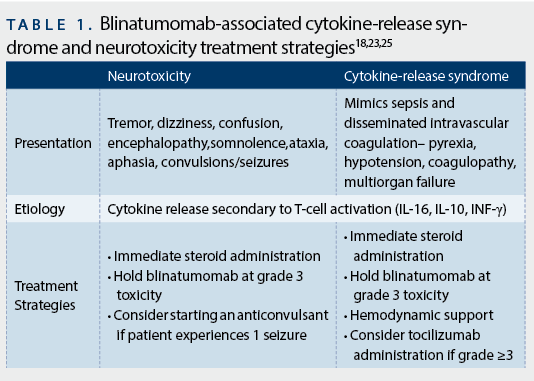
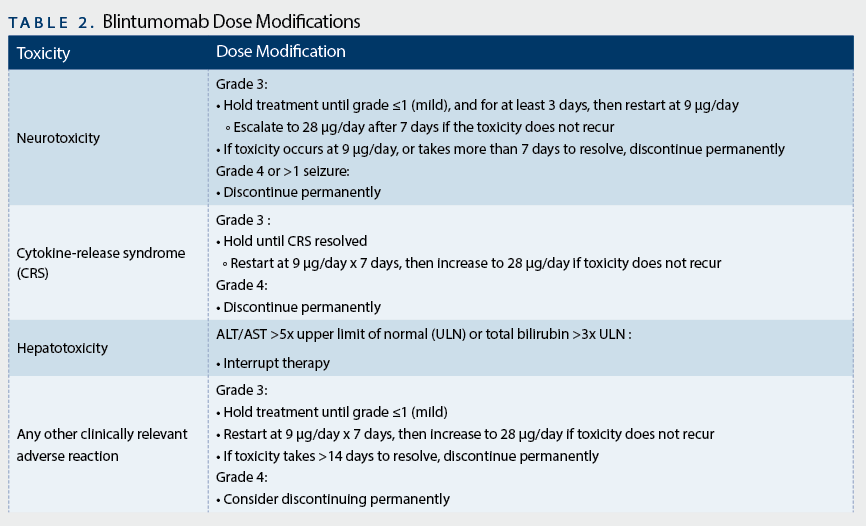
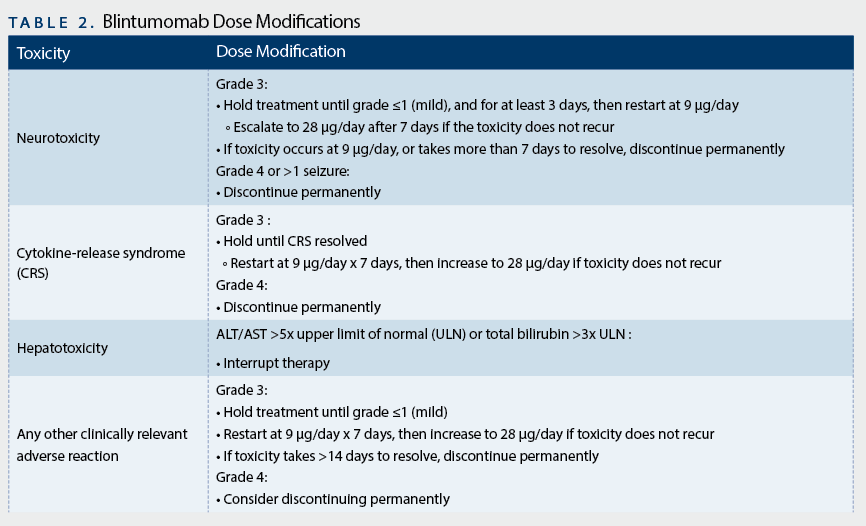
The most serious AEs associated with blinatumomab are CRS and neurologic toxicity, both associated with black box warnings and have prompted a Risk Evaluation and Mitigation Strategy (REMS) program to inform health care providers (HCP) about these risks. Manifestations of severe CRS mimic that of sepsis and disseminated intravascular coagulopathy; patients can experience severe pyrexia, hypotension, coagulopathy, and multiorgan failure. Patients with CRS are known to have elevations of proinflammatory cytokines, specifically IL-6, IL-10, and INF-γ, during the height of T-cell activation.17,23While both nonsteroidal anti-inflammatory drugs and steroids can inhibit increases in cytokine levels, dexamethasone did not appear to effect blinatumomab-mediated cytotoxicity, since there was no notable effect of dexamethasone prephase on blinatumomab response in the large Topp trial.22While CRS events were observed at higher rates in earlier blinatumomab studies, implementation of a dose-step approach during the first cycle, dexamethasone premedication, and a required steroid prephase for patients with high tumor burden have reduced the rates of severe CRS. However, given the risk for serious CRS, close monitoring of patients when initiating treatment and with any dose escalation is critical.TABLE 2highlights important recommendations for dose modifications.

Other strategies used to manage CRS include targeting the cytokines directly, specifically targeting IL-6 given the high amounts released with blinatumomab administration.24Tocilizumab, a recombinant humanized monoclonal antibody against the IL-6 receptor, approved for rheumatoid and juvenile idiopathic arthritis, has recently been used for the management of CRS. Patients treated with blinatumomab who develop grade 3 or greater CRS refractory to steroids and are treated with tocilizumab typically see resolution of symptoms within hours,25making it a treatment that should be considered for patients with steroid-refractory blinatumomab-induced CRS. However, tocilizumab has not been prospectively evaluated in a clinical trial and future studies are warranted to provide a better understanding about its role in CRS management, given that it could potentially blunt T-cell proliferation by interfering with cytokine feedback loops, possibly compromising the efficacy of blinatumomab.
Neurotoxicity related to blinatumomab use is seen significantly more than CRS. In the Topp study,2252% of patients (n = 98/189) experienced neurologic toxicities, which included tremor, dizziness, confusion, encephalopathy, somnolence, ataxia, and aphasia. This risk increased in patients ≥65 years of age. Neurologic events were predominately grade 1-2, typically occurred in cycle 1, and were treated with dexamethasone without interruption of blinatumomab. However, of the 98 patients who experienced neurologic toxicities, 29 required treatment interruptions. In the smaller phase II study,21patients with epilepsy or convulsions were successfully resumed on blinatumomab with the addition of an anticonvulsant. Because of this warning, the manufacturer recommends that patients avoid operating machinery or motor vehicles while being treated with blinatumomab. While the mechanism behind the neurotoxicity remains largely unknown, it has been hypothesized to be IL-6 directed,25which would not be ameliorated with tocilizumab given its lack of penetration across the blood-brain barrier. Strict monitoring and prompt initiation of steroids are critical in preventing and treating neurotoxicity while continuing blinatumomab. However, dose interruption may also be warranted.
Blinatumamab also carries a warning about hepatotoxicity. Grade ≥3 increases in aspartate transaminase (AST), alanine transaminase (ALT) and/or bilirubin were seen in >10% of patients early in treatment and may have been associated with cytokine release. Nearly all increases in liver enzymes resolved with treatment continuation or interruption, and patients who had therapy interrupted were successfully rechallenged.26Other AEs are reported inTABLE 3.


Drug Interactions
While blinatumomab has not been shown to directly affect CYP450 enzyme activity in vitro, there is an indirect effect that may occur because of the transient cytokine elevation seen with blinatumomab use. The cytokine elevation and maximal CYP suppression potential are expected to occur during the first 9 days of the first cycle and the first 2 days of the second cycle. Therefore, patients who are on medications with a narrow therapeutic index should be closely monitored for toxicity during this period of treatment.17,18
Dosage and Administration
The dosing instructions for blinatumomab are summarized inTABLE 4. Blinatumomab is given IVCI for 28 consecutive days followed by 2 treatment-free weeks. The 2-week treatment- free interval between cycles is used because of the decrease of activated T cells seen after expansion in previous studies.27Patients may receive two induction cycles (cycles 1 and 2) followed by three consolidation cycles if in CR/CRh (cycles 3-5). A dose-step approach is used in cycle 1 to minimize AEs. Patients should be premedicated with dexamethasone 20 mg IV 1 hour before the first dose of blinatumomab in each cycle, prior to an increase in dose, or when restarting an infusion that has been interrupted for ≥4 hours. Patients must be hospitalized for the initial 9 days of cycle 1 and the first 2 days of cycle 2. When treated as outpatient, patients must return every 24 or 48 hours for bag exchange.

Preparation of blinatumomab differs depending on the dose and bag size (24-hour or 48-hour bag). Because of reported medication errors (including underdosing and overdosing) during clinical trials, an REMS program has been established. The manufacturer provides specific preparation/admixing and administration instructions that must be strictly followed. Blinatumomab is available in a 35-µg vial that also contains 10 mL of an IV solution stabilizer (IVSS), allowing for single use only. Per the manufacturer, blinatumomab must be put in 250-mL polyolefin, PVC non-di-ethylhexyl phthalate (non-DEHP), or ethyl vinyl acetate (EVA) infusion bags or pump cassettes with 0.9% sodium chloride. The IVSS should be transferred to the 250-mL bag before adding the drug to prevent drug adhesion to the bag itself. The overfill of the 250-mL 0.9% sodium chloride bag should not be removed to reduce the amount of manipulations, as well as adhering to the concentration being infused. The total amount of blinatumomab added to the prepared bag will be more than the 9 µg or 28 µg the patient is to receive in a 24-hour period−this is to account for the overfill and the standardized rate of administration. The IV line should be sterile, nonpyrogenic, low protein binding, with a 0.2 micron filter and primed with drug. Blinatumomab needs to be infused in a dedicated line and should not be flushed. Any unused drug from the bag or IV line should be discarded at the end of infusion to prevent administering a bolus of the medication.
If blinatumomab administration is held for 4 hours or more, patients must be under the supervision of an experienced HCP to restart the infusion, and dexamethasone 20 mg IV should be given before restarting the infusion. Often, this requires a hospitalization. Thus, it is important to avoid ≥4-hour delay in therapy.
If blinatumomab is interrupted for less than 7 days, it is recommended to continue the same cycle to a total of 28 days of infusion, inclusive of days before and after the interruption in that cycle. If the interruption is greater than 7 days, a new cycle must be started.
Discussion and Future Directions
Blinatumomab has emerged as a novel and effective salvage treatment for adult patients with relapsed or refractory B-ALL, a population with limited treatment options and a dismal prognosis. Allogeneic HSCT is the only potentially curative treatment but is associated with significant morbidity and mortality, particularly in patients who are elderly, with comorbidities, and/or with resistant or high-risk disease. Historically, 30%-45% of patients experience a CR with first salvage therapy consisting of high-dose combination chemotherapy2,3,5; this percentage is significantly lower with each subsequent salvage and is associated with significant mortality.28Vincristine sulfate liposome injection (VSLI), which is relatively new to the market, was approved as monotherapy for adult patients with Ph- ALL whose disease progressed after 2 or more therapies based on a CR/CRh rate of 20%.29In comparison, 43%-69% of patients treated with blinatumomab achieved CR/CRh and 40%-52% of patients underwent subsequent HSCT in the phase II studies,22,23showing blinatumomab’s promising potential as a bridge to transplantation. A phase III trial is underway of blinatumomab versus investigator’s choice of chemotherapy in patients with relapsed/refractory B-ALL.30
Blinatumomab has a notable effect on inducing MRD-negativity, in both the salvage and upfront settings. More than 80% of patients with relapsed/refractory B-ALL achieved MRD negativity in the salvage setting, which correlated with a longer RFS and OS.22,23Additionally, in an earlier blinatumomab phase II trial, 21 adult patients with ALL in CR after induction and consolidation therapy, but with MRD positivity, were treated with blinatumomab in the front-line setting. Of the 20 evaluable patients, 80% achieved MRD negativity within 4 cycles.31After a follow-up of 33 months, 12 patients remained in CR, with a hematologic RFS of 61%.32Of the 6 patients with Ph- MRD negativity, 4 went on to have hematologic and molecular remission with no subsequent therapy. However, there was no significant difference in long-term disease control in patients who subsequently underwent HSCT (9 of the original 20 patients) and those who did not. The role of blinatumomab as consolidation therapy for patients with newly diagnosed Ph- B-ALL is being further explored in an ongoing phase III trial.33
Although not approved for the treatment of Ph+ B-ALL, response rates have been demonstrated in some patients who were Ph+ and were treated with blinatumomab.21Additionally, there is an ongoing phase II trial with single-agent blinatumomab in adult patients with Ph+ relapsed/refractory B-ALL.34. The NCCN lists blinatumomab as a possible treatment option for patients with Ph+ precursor B-cell ALL refractory or intolerant to TKIs.7Other areas of investigation include front-line treatment in combination with low-dose chemotherapy (with or without TKI) for elderly patients with Ph+ or Ph- B-ALL.35
While the risk of CRS and neurologic toxicities is significant, incorporating a dexamethasone prephase and vigilant monitoring during initiation have significantly reduced the risk of severe toxicities without knowingly compromising efficacy.
Given the potentially serious toxicities, strict monitoring required, and the complicated preparation and administration requirements, NCCN recommends patients be treated at a specialized cancer center with experience administering blinatumomab. Furthermore, a collaborative effort with multidisciplinary involvement and communication is vital to ensuring blinatumomab administration is done correctly and safely.
Administration logistics may pose an obstacle for institutions that administer blinatumomab. Administration calls for IVCI for 28 consecutive days every 6 weeks, which requires both hospitalization and for patients to return for bag exchanges every 24 or 48 hours on discharge, or to establish home health care visits by a HCP with blinatumomab experience. It is also crucial to avoid delays in therapy of ≥4 hours.
Finally, the cost of blinatumomab is worth discussing; the median number of cycles administered to patients in the Topp 2014 phase II study was ~1.5. A 35-µg vial at the average wholesale price (AWP) is $3,814, with 1 cycle ranging anywhere from $52,000 to $103,000, depending on the frequency of blinatumomab drug replacement (24 hours vs 48 hours preparations). In comparison, the AWP of 5 mg of liposomal vincristine runs at $12,630; patients received a median of 4 doses in the phase II study that won FDA approval to liposomal vincristine, averaging a cost of $50,000.36
Conclusion
Blinatumomab’s unique mechanism of action and robust activity shown in the phase II trials make it a promising option for patients with B-ALL who have failed or relapsed from first-line therapy. In light of its approval through the FDA’s accelerated approval pathway, further studies will determine its ultimate place in therapy for ALL and other lymphoid malignancies. Because of the serious toxicities associated with blinatumomab, such as CRS and neurologic toxicities, patients require close monitoring and early management of toxicities. Lastly, with other new immunotherapies, such as chimeric antigen receptor T-cell therapies and inotuzumab ozogamicin showing favorable outcomes, comparative trials with these therapies should be considered to further define the role of blinatumomab in precursor B-ALL.
Declaration of Conflicting Interests
Daniel Wojenski is on the speaker’s bureau for Sanofi Oncology.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015.Ca Cancer J Clin. 2015;65:5-29.
- Oriol A, Vives S, Hernandez-Rivas JM, et al. Outcome after relapse of acute lymphoblastic leukemia in adult patients induced in four consecutive risk adapted trials by the PETHEMA study group.Hematologica. 2010;95(4):589-596.
- Gokbuget N, Stanze D, Beck J, et al. Outcome of relapsed adult lymphoblastic leukemia depends on response to salvage chemotherapy, prognostic factors, and performance of stem cell transplantation.Blood. 2012;120(10):2032-2041.
- Pulte D, Jansen L, Gondos A, et al. Survival of adults with acute lymphoblastic leukemia in Germany and in the United States.PLoS ONE.2014;9:e85554.
- Kantarjian HM, Thomas D, Ravandi F, et al. Defining the course and prognosis of adults with acute lymphocytic leukemia in first salvage after induction failure or short first remission duration.Cancer. 2010;116(24):5568-5574.
- Faderi S, Thomas DA, O’Brien S, et al. Augmented hyper-CVAD based on dose-intensified vincristine, dexamethasone, and asparaginase in adult acute lymphoblastic leukemia salvage therapy.Clin Lymphoma Myeloma Leuk.2011;11:54-59.
- National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology: Acute Lymphobastic Leukemia (V2.2014). http://www.nccn.org/professionals/physician_gls/pdf/all.pdf. Accessed April 3, 2015.
- US Food and Drug Administration. December 3, 2014. FDA approves Blincyto to treat a rare form of acute lymphoblastic leukemia [news release]. Retrieved from http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm425549.htm. Accessed April 3, 2015.
- Baeuerle PA, Kufer P, Bargou R. BiTE: Teaching antibodies to engage T-cells for cancer therapy.Curr Opin Mol Ther. 2009;11:22-30.
- Baeuerle PA, Reinhardt C. Bi-specific T-cell engaging antibodies for cancer therapy.Cancer Res.2009;69:4941-4944.
- Nagorsen D, Baeuerle PA. Immunomodulatory therapy of cancer with T cell engaging BiTE antibody blinatumomab.Exp Cell Res.2011;317:1255-1260.
- Alberts B, Johnson A, Lewis J, et al. Molecular Biology of the Cell. 4th ed. New York: Garland Science; 2002. T Cells and MHC Proteins. Available from: http://www.ncbi.nlm.nih.gov/books/NBK26926/.
- Tedder TF, Zhou LJ, Engel P. The CD19/CD21 signal transduction complex of B lymphocytes.Immunology. 1994;15(9):437-442.
- Fujimoto M, Fujimoto Y, Poe JC, et al. CD19 regulates Src family protein tyrosine kinase activation in B lymphocytes through processive amplification.Immunity. 2000;13:47-57.
- Wu B, Hijazi Y, Wolf A, et al. Pharmacokinetics of blinatumomab and its clinical implications. ASCO Meeting. 2013;31: Abstract 3048.
- Nagorsen D, Kufer P, Baeuerle PA, et al. Blinatumomab: A historical perspective.Pharm Ther.2012;136:334-342.
- Center for Drug Evaluation and Research. Clinical Pharmacology and Biopharmaceutics Reviews: Application 125557Orig1s000. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/125557Orig1s000ClinPharmR.pdf. Accessed April 3, 2015.
- BLINCYTO[package insert]. Thousand Oaks, CA: Amgen Inc; 2014.
- Hijazi Y, Klinger M, Schub A, et al. Blinatumomab exposure and pharmacodynamic response in patients with non-Hodgkin lymphoma (NHL) [abstract].J Clin Oncol. 2013;31: Abstract 3051.
- Zhu M, Kratzer A, Johnson J, et al. Pharmacokinetics/pharmacodynamics of blinatumomab in patients with relapsed/refractory B-precursor acute lymphoblastic leukemia [abstract].J Clin Oncol.2015;33: Abstract 2561.
- Topp MS, Gokbuget N, Zugmaier G, et al. Phase II trial of the anti-CD19 bispecific T cell engager blinatumomab shows hematologic and molecular remission in patients with relapsed or refractory B-precursor acute lymphocytic leukemia.J Clin Oncol. 2014;32(36):4134-4140.
- Topp MS, Gokbuget N, Stein AS, et al. Safety and activity of blinatumomab for adult patients with relapsed or refractory B-precursor acute lymphoblastic leukemia: a multicentre, single-arm, phase 2 study.Lancet Oncol. 2015;16:57-66.
- Maude SL, Barett D, Teachey DT, et al. Managing cytokine release syndrome associated with novel T cell engaging therapies.Cancer J.2014;20(2):119-122.
- Teachey DT, Rheingold SR, Maude SL, et al. Cytokine release syndrome after blinatumomab treatment related to abnormal macrophage activation and ameliorated with cytokine-directed therapy.Blood. 2013;121(26):5154-5157.
- Lee DW, Gardner R, Porter DL, et al. Current concepts in the diagnosis and management of cytokine release syndrome.Blood. 2014;124(2):188-195.
- Center for Drug Evaluation and Research. Medical Reviews: Application 125557Orig1s000. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/125557Orig1s000MedR.pdf. Accessed April 3, 2015.
- Bargou R, Leo E, Zugmaier G, et al. Tumor regression in cancer patients by very low doses of a T cell-engaging antibody.Science. 2008;321:974-977.
- O’Brien S, Thomas D, Ravandi F, et al. Outcome of adults with acute lymphocytic leukemia after second salvage therapy.Cancer. 2008:113;3186-3191.
- O’Brien S, Schiller G, Lister J, et al. High-dose vincristine sulfate liposome injection for advanced, relapsed, and refractory adult Philadelphia chromosomenegative acute lymphoblastic leukemia.J Clin Oncol. 2013;31(6):676-683.
- Amgen. Ph 3 trial of blinatumomab vs investigator’s choice of chemotherapy in patients with relapsed or refractory ALL. In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2000-[cited 2015 Sept 25]. Available from:https://clinicaltrials.gov/ct2/show/NCT02013167.
- Topp MS, Kufer P, Gokbuget N, et al. Targeted therapy with the T-cellengaging antibody blinatumomab of chemotherapy-refractory minimal residual disease in B-lineage acute lymphoblastic leukemia patients results in high response rate and prolonged leukemia-free survival.J Clin Oncol. 2011;29:1-6.
- Topp MS, Gokbuget N, Zumaier G, et al. Long-term follow-up of hematologic relapse-free survival in a phase 2 study of blinatumomab in patients with MRD in B-lineage ALL.Blood. 2012;120(26):5185-5187.
- National Cancer Institute. Combination chemotherapy with or without blinatumomab in treating patients with newly diagnosed BCR-ABL-negative B lineage acute lymphoblastic leukemia. In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2000-[cited 2015 Oct 5]. Available from: https://clinicaltrials.gov/ct2/show/NCT02003222.
- Amgen. Phase 2 trial of blinatumomab in Philadelphia positive/BCR-ABL positive acute lymphoblastic leukemia. In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2000-[cited 2015 Sept 25]. Available from: https://clinicaltrials.gov/ct2/show/NCT02000427.
- National Cancer Institute. Blinatumomab and combination chemotherapy or dasatinib, prednisone, and blinatumomab in treating older patients with newly diagnosed acute lymphoblastic leukemia. In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2000-[cited 2015 Sept 25]. Available from:https://clinicaltrials.gov/ct2/show/NCT02143414.
- Redbook Online [online database]. Greenwood Village, CO: Truven Health Analytics (accessed 2015 Sept 24).










Novel Approaches Focus on Limiting Toxicity in Older Patients With ALL
April 22nd 2024The major challenges for clinicians treating older patients with acute lymphoblastic leukemia surround the emergence of resistance to existing therapies and the toxicities associated with current chemotherapies.
Read More


Ornstein Advises on Starting Dose and Management of Lenvatinib in RCC
April 21st 2024During a Case-Based Roundtable® event, Moshe Ornstein, MD, MA, provided guidance on dosing and toxicity concerns in a patient treated with lenvatinib plus pembrolizumab for advanced renal cell carcinoma.
Read More

Rugo Surveys Peers on Treatment After Metastatic Relapse of HR+, HER2– Breast Cancer
April 20th 2024During a Case-Based Roundtable® event, Hope S. Rugo, MD, FASCO, moderated a discussion on treatment options for a patient whose breast cancer recurred several years after adjuvant therapy.
Read More

