ADCs Stake Their Claim in Lymphoma Paradigm
Antibody–drug conjugate therapies are making a larger impact on the treatment paradigm for patients with lymphomas, especially following promising data for brentuximab vedotin and inotuzumab ozogamicin.
Brad Kahl, MD
Antibodydrug conjugate (ADC) therapies are making a larger impact on the treatment paradigm for patients with lymphomas, especially following promising data for brentuximab vedotin (Adcetris) and inotuzumab ozogamicin (Besponsa).
“The rationale for ADCs is quite self-evident,” said Brad Kahl, MD. “The goal is to deliver cytotoxic agents, and to deliver them more selectively. If you are able to achieve that, you can improve the therapeutic index, which would then, in theory, allow for the delivery of more potent cytotoxic agents that you could administer intravenously.”
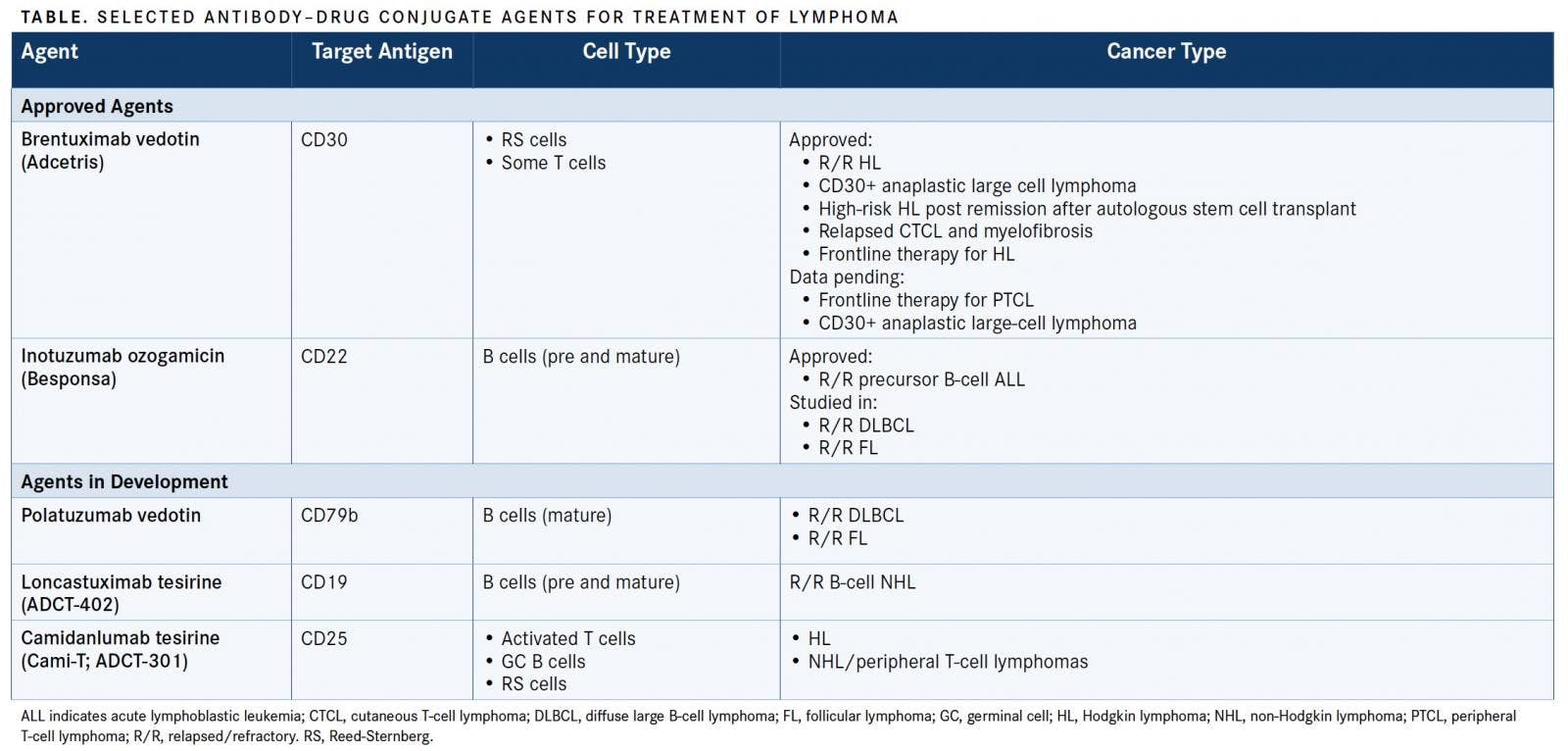
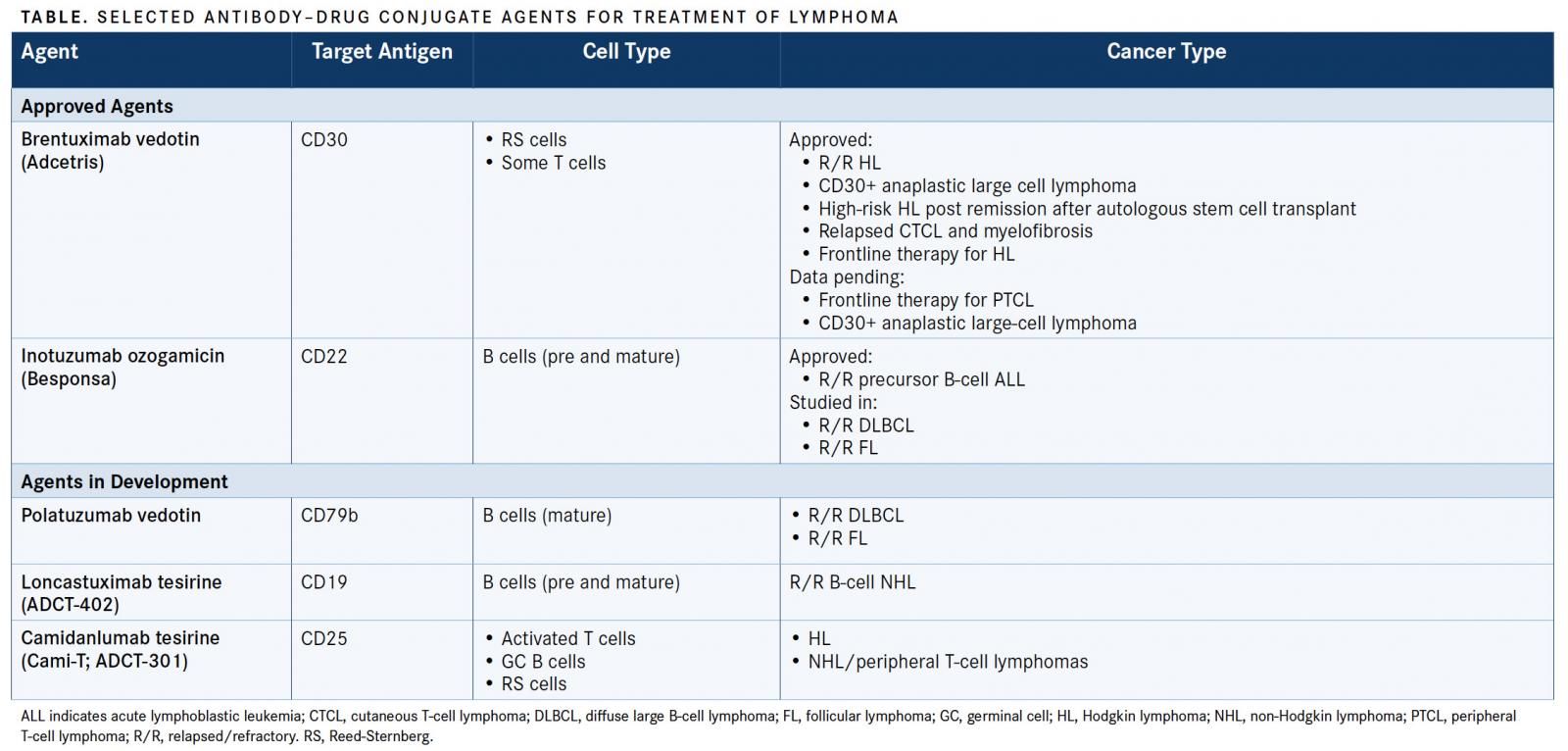
In a presentation on new ADCs during the 2018 Pan Pacific Lymphoma Conference, Kahl described the current use of ADCs in lymphomas, as well as novel agents in later-stage development (TABLE). He is a professor in the Department of Medicine, Washington University School of Medicine in St. Louis, and a medical oncologist at the Siteman Cancer Center.
ADC Building Blocks
To build an ADC, there must first be an antigenantibody combination, then a linker, a conjugation, and finally a payload, Kahl explained. “Antigens should be tumor-specific, internalized, and abundantsomedata suggest that 10,000 antigens per tumor cell is the minimum. Then, you need a good monoclonal antibody to bind to that antigen,” said Kahl.
Examples of target antigens for ADCs currently under evaluation include CD19, CD22, CD25, CD30, CD37, and CD79b.
Linkers are short chemical spaces that bind the antibody to the drug, explained Kahl. The linker ends up being very important in the construction of an ADC, as it must be stable in circulation to inhibit the agent from moving freely in the patient. These linkers must be able to release the drug upon internalization, Kahl said.
There are 2 types of linkers: cleavable and noncleavable. Cleavable linkers include hydrazones, which release the payload under acid conditions of the lysosome; disulfides, which undergo thiol-disulfide exchange reactions; and peptides, which release the payload after protease cleavage. Noncleavable linkers allow the entire ADC to be degraded in a lysosome-releasing payload. These linkers are theoretically more stable in circulation, Kahl explained.
Conjugation focuses on the drug-to-antibody ratio (DAR). If too little drug is in the antibody, potency can be lost; however, if there is too much, it can result in increased toxicity or hydrophobicity. Some data suggest that a DAR of 4 is optimal, said Kahl.
There are different ways to place the drug onto the antibody, he added. The heterogeneous payload placement method is the most common. It exploits the endogenous lysine or hinge cysteine residues.
This is a nonspecific way to get the drug onto the antibody, as the DAR ranges from 0 to 8 per antibody, but it is more commonly used.
There is also the site-specific method, in which reactive chemical handles are placed on the monoclonal antibody. This results in more control of the DAR, Kahl said. Some newer ADCs in development are using this method.

Among the payloads used in ADCs are microtubule inhibitors, such as auristatins and maytansines. Others are DNA-damaging agents such as enediynes, duocarmycin derivatives, and pyrrolobenzodiazepines. Toxins can also be used, Kahl said, such as pseudomonas exotoxin and ricin.
“It is estimated that less than 2% of the payload administered actually localizes to the tumor cell when you are administering ADCs,” Kahl said. “So, your payload must be very potent.”
ADCs in the Landscape
Brentuximab vedotin has been approved for use in patients with relapsed or refractory (R/R) Hodgkin lymphoma, CD30-positive anaplastic large cell lymphoma, high-risk Hodgkin lymphoma post remission after autologous stem cell transplant, relapsed cutaneous T-cell lymphoma and myelofibrosis, and as a frontline therapy for Hodgkin lymphoma. The major toxicities associated with brentuximab vedotin include neuropathy, nausea, and fatigue.
Inotuzumab ozogamicin was approved by the FDA in 2017 for R/R precursor B-cell acute lymphocytic leukemia. It is currently being evaluated in R/R diffuse large B-cell lymphoma (DLBCL) and R/R follicular lymphoma. Significant toxicities linked with this ADC include myelosuppression, nausea, and fatigue.
Polatuzumab vedotin, a CD79b humanized monoclonal antibody cleavable peptide linker, is currently being investigated as a single agent, in combination with rituximab (Rituxan), and in combination with bendamustine (Treanda) and rituximab (BR). It is also being tested in combination with rituximabcyclophosphamide, doxorubicin, and prednisone versus rituximab– cyclophosphamide, doxorubicin, vincristine, and prednisone with placebo in the POLARIX trial (NCT03274492).
Patients with R/R follicular lymphoma and DLBCL are being evaluated in a randomized phase II trial of polatuzumab vedotin plus BR (NCT02257567). In the study, polatuzumab is given at a dose of 1.8 mg/kg once daily with 90 mg/m2 of intravenous (IV) bendamustine every 2 days, and 375 mg/m2 of IV rituximab once daily. The patients with follicular lymphoma (n = 80) are undergoing six 28-day cycles, while those with DLBCL are undergoing six 21-day cycles.
Kahl explained that the conclusions drawn from this trial thus far are that polatuzumab vedotin can be safely administered in combination with BR. There was no significant difference with short-term follow-up for patients with follicular lymphoma, but adding polatuzumab vedotin to BR improved response rates, progression-free survival (HR, 0.31; 95% CI, 0.18-0.55; P <.0001), and overall survival (HR, 0.35; 95% CI, 0.19-0.67; P = .0008) in the DLBCL group regardless of prior lines of treatment or whether patients had refractory disease.1
In 2017, the FDA granted a breakthrough therapy designation to polatuzumab vedotin for the treatment of patients with R/R DLBCL. The European Medicines Agency also granted the ADC a priority medicines designation.
“If it were to get approved at some point, it would certainly be an attractive option for patients with relapsed large cell lymphoma who are in palliative mode, and [are unable to be treated] with curative intent anymore,” Kahl said.
ADCs Under Investigation
Loncastuximab tesirine (Lonca-T; ADCT-402), a novel pyrrolobenzodiazepine-based ADC, is currently being evaluated in patients with R/R B-cell lineage non-Hodgkin lymphoma (NCT02669017).
“This is an ADC that was interesting because of the payload it uses. It is an antibody that targets CD19. It has its linker, but the payload in this case is this p-phenylenediamine [PPD] dimer, which is a highly potent cytotoxic agent,” explained Kahl. “The company [ADC Therapeutics] feels that because they used a stochastic conjugation technology, that they can more tightly control the number of payload molecules per antibody, which can result in better pharmacokinetic properties and a better safety profile.”
Treatment-related adverse events observed in the phase I dose-escalation study of Lonca-T include skin-related changes, fatigue, nausea, increased gamma-glutamyl transferase (GGT), anemia, and peripheral edema, according to interim results from the first-in-human clinical study that Kahl presented during the 2017 American Society of Hematology Annual Meeting.2
Patients were treated with doses of Lonca-T ranging from 15 to 200 μg/kg for a median of 2 cycles (range, 1-16). In patients with DLBCL, the overall response rate (complete + partial responses) was 49.1% across all doses (n = 59) and 55.1% among those who received the drug at ≥120 μg/kg.
Camidanlumab terisine (Cami-T; ADCT-301), a CD25 monoclonal antibody protease cleavable linker PPD dimer, is being investigated in an ongoing phase I/II trial in Hodgkin lymphoma and non-Hodgkin lymphoma (NCT02432235). In preliminary data, investigators reported that the overall response rate observed with this agent in patients with Hodgkin lymphoma was 71% (n = 35); it was 33% (n = 12) in patients with peripheral T-cell lymphoma. The toxicities observed so far include rash, edema, and GGT elevation. In this study, 2 cases of Guillain-Barré syndrome were observed.3
Additional novel ADCs under investigation include A-dmDT390-bisFv(UCHT1), known by the trade name Resimmune, coltuximab ravtansine (SAR3419), denintuzumab mafodotin (SGNCD19A), pinatuzumab vedotin (DCDS4501A), moxetumomab pasudotox, and naratuximab emtansine (IMGN529). Currently, no clinical trials listed on ClinicalTrials.gov are recruiting patients.4
“A lot of considerations go into making an ADC, and the linker technology and the conjugation strategy just may turn out to be the most important part of all of this to optimize the therapeutic index for ADCs,” concluded Kahl.
References:
- Sehn LH, Kamdar M, Herrera AF, et al. Randomized phase 2 trial of polatuzumab vedotin (pola) with bendamustine and rituximab (BR) in R/R (R/R) FL and DLBCL. J Clin Oncol. 2018;36(suppl; abstr 7507). meetinglibrary.asco. org/record/159486/abstract.
- Kahl BS, Hamadani M, Caimi P, et al. Encouraging early results from the first in-human clinical trial of ADCT-402 (loncastuximab tesirine), a novel pyrrolobenzodiazepine-based antibody drug conjugate, in R/R B-cell lineage non-Hodgkin lymphoma. Blood. 2017;130(suppl 1):187. bloodjournal.org/ content/130/Suppl_1/187.
- Horwitz SM, Hamadani M, Fanale MA, et al. Interim results from a phase 1 study of ADCT-301 (camidanlumab tesirine) show promising activity of a novel pyrrolobenzodiazepine-based antibody drug conjugate in R/R Hodgkin/ non-Hodgkin lymphoma. Blood. 2017;130(suppl 1):1510. bloodjournal. org/content/130/Suppl_1/1510.
- NIH clinical trials database. ClinicalTrials.gov website. Accessed August 17, 2018.












Examining the Non-Hodgkin Lymphoma Treatment Paradigm
July 15th 2022In season 3, episode 6 of Targeted Talks, Yazan Samhouri, MD, discusses the exciting new agents for the treatment of non-Hodgkin lymphoma, the clinical trials that support their use, and hopes for the future of treatment.
Listen



