Immunotherapy Combinations Are Changing the Frontline Treatment of Patients With NSCLC
Checkpoint inhibitors are revolutionizing the treatment of patients with both squamous and nonsquamous non-small cell lung cancer, and are quickly assuming a predominant role, especially in the frontline setting, due to recent exciting results from large trials.<br />
Julian R. Molina, MD, PhD
Just 3 years ago, nivolumab (Opdivo) became the first checkpoint inhibitor approved for the treatment of nonsmall cell lung cancer (NSCLC).1Less than half a decade later, 4 checkpoint inhibitors2 antiPD-1 antibodies, nivolumab and pembrolizumab (Keytruda), and 2 anti– PD-L1 therapies, atezolizumab (Tecentriq) and durvalumab (Imfinzi)—have been approved by the FDA to treat NSCLC. These agents are revolutionizing the treatment of patients with both squamous and nonsquamous NSCLC, and are quickly assuming a predominant role, especially in the frontline setting, due to recent exciting results from large trials.1
“It’s been incredible how quickly this has happened,” Lauren Byers, MD, associate professor of thoracic and head and neck medical oncology at The University of Texas MD Anderson Cancer Center, said in an interview with Targeted Therapies in Oncology. “I can’t think of many times in our field where there have been multiple high-impact papers coming out all around the same time, at 1 major meeting after the next. This will shift the standard treatment for the majority of our patients.”
Recent advances in checkpoint inhibition have been driven by the desire to improve outcomes for patients and families. Early immunotherapy trials demonstrated tremendous benefit, but only for some patients. The phase III KEYNOTE-024 trial of pembrolizumab versus standard chemotherapy, showed that pembrolizumab alone was more effective (and better tolerated) than chemotherapy, but only in patients who demonstrated at least 50% PD-L1 expression.2Unfortunately, only about 30% of patients with NSCLC have PD-L1 levels greater than 50%, said Julian R. Molina, MD, PhD, a professor of oncology at Mayo Clinic. “The question became, well, how are we going to treat the ones that have less than 50% PD-L1 expression?” Molina said.
Data from a few recently published and presented studies may answer this question. According to Molina, “What you see from the [data of] clinical trials presented at the 2018 ASCO Annual Meeting is that the combination of chemotherapy plus immunotherapy seems to be useful and results in good outcomes. Based on the evidence that is out there right now, chemotherapy alone is not the best treatment for a patient with newly diagnosed lung cancer. You have to give chemotherapy in combination with immunotherapy, or immunotherapy alone, depending on the PD-L1 levels, or an inhibitor if they have a driver mutation.”
Nonsquamous NSCLC
According to the recentSociety for Immunotherapy of Cancer’s (SITC) consensus statements on immunotherapy for the treatment of NSCLC, pembrolizumab monotherapy should be used as first-line therapy in patients with PD-L1positive nonsquamous metastatic NSCLC.1First-line treatment with pembrolizumab plus pemetrexed (Alimta) and carboplatin may also be appropriate for these patients on a case-by-case basis. Patients with a PD-L1 tumor proportion score (TPS) less than 50% and no actionable mutations should receive first-line pembrolizumab with pemetrexed and carboplatin.
The promising results from several trials presented at major meetings in the past few months have received a great deal of attention for their potential impact on treatment for patients with nonsquamous NSCLC (TABLE 1).

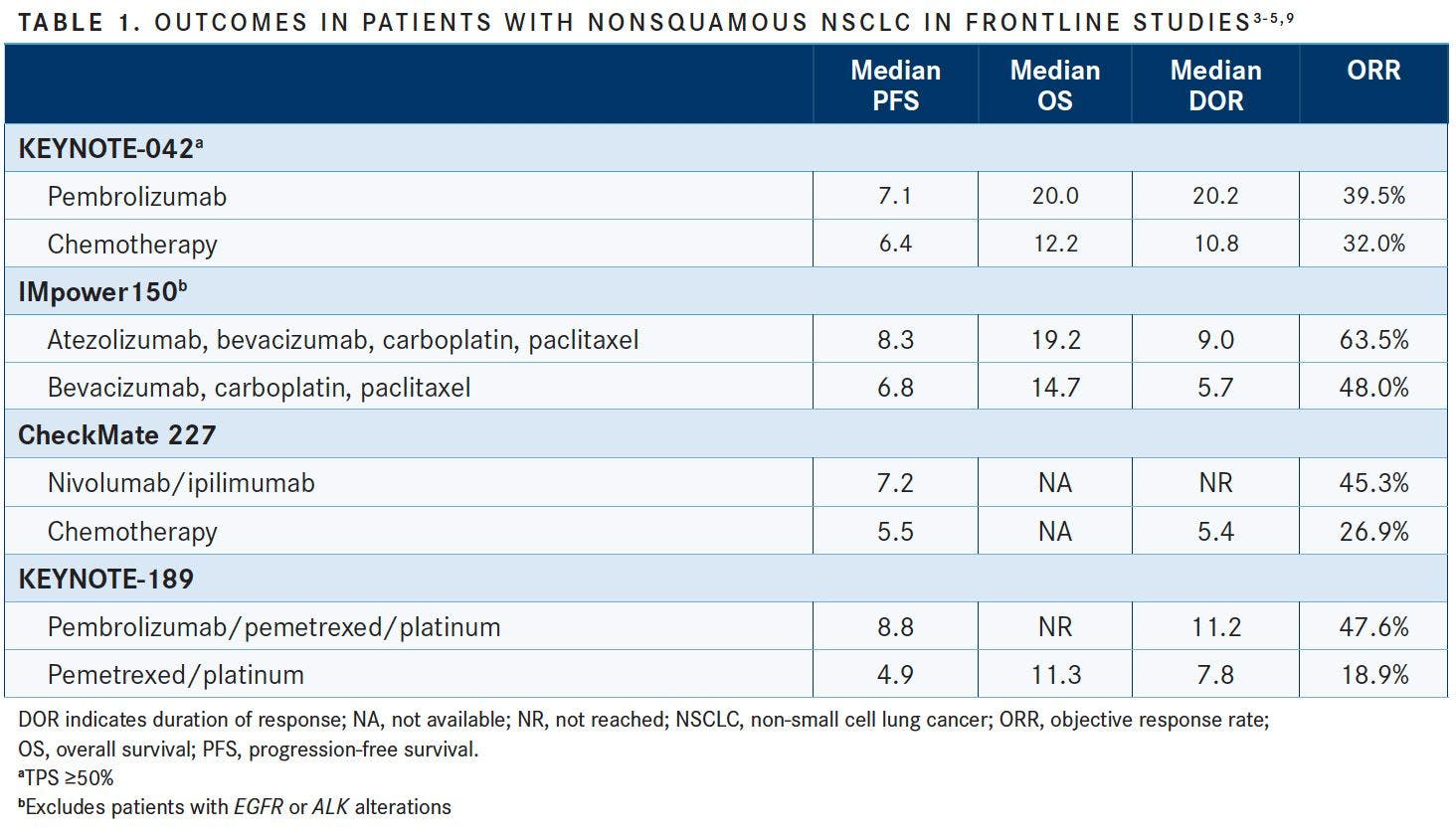
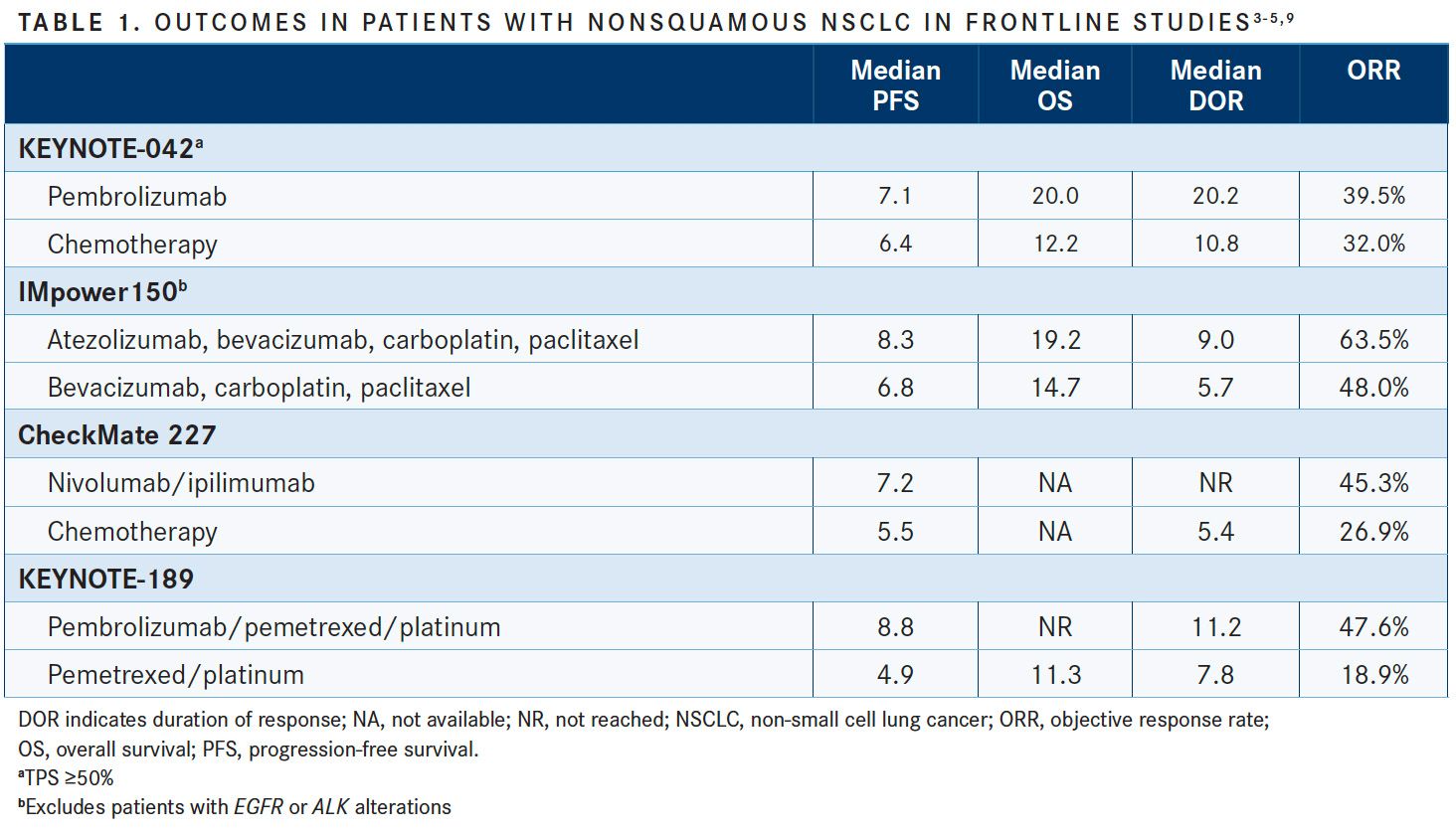
KEYNOTE-042 compared pembrolizumab to platinum-based chemotherapy as a first-line therapy for patients with advanced or metastatic NSCLC and a PD-L1 TPS of ≥1%. Patients received up to 35 cycles of pembrolizumab 200 mg every 3 weeks or the investigator’s choice of up to 6 cycles of paclitaxel/carboplatin or pemetrexed/carboplatin with optional pemetrexed maintenance.3Those who received pembrolizumab alone lived a median of 4 to 8 months longer than those who received chemotherapy.
In patients with TPS ≥1%, the median overall survival (OS) was 16.7 months (95% CI, 13.9-19.7) with pembrolizumab compared with 12.1 months (95% CI, 11.3-13.3) with chemotherapy (HR, 0.81; 95% CI, 0.71-0.93; P = .0018). The OS results were even more pronounced in the higher TPS groups: in patients with TPS ≥20%, the median OS was 17.7 months (95% CI, 13.3-22.1) versus 13.0 months (95% CI, 11.6-15.3) (HR, 0.77; 95% CI, 0.64-0-.92; P = .0020), and 20.0 months (95% CI, 15.4-24.9) versus 12.2 months (95% CI, 10.4-14.2) in those with TPS ≥50%, respectively (HR, 0.69; 95% CI, 0.56-0.85; P = .0003).
Severe adverse events (AEs) were less common in the pembrolizumab group compared with chemotherapy (17.8% vs 41.0%, respectively), but there were more severe immune-mediated AEs and infusion reactions with pembrolizumab (8.0% vs 1.5%).3
“For most nonsquamous patients, the question now is, can the patient get pembrolizumab by itself, or should they get pembrolizumab in combination with carboplatin and pemetrexed?” Byers said. She often recommends pembrolizumab only to elderly or medically frail patients who may find it difficult to tolerate chemotherapy. For patients with a high PD-L1 level, “whenever possible, I do want to add chemotherapy because I think they may get a faster response,” Byers stated, noting that additional research is needed to determine whether there is greater benefit in sequencing pembrolizumab and chemotherapy, or giving them simultaneously.
The phase III IMpower150 clinical trial is investigating the use of atezolizumab plus bevacizumab (Avastin) plus carboplatin and paclitaxel chemotherapy in patients with metastatic nonsquamous NSCLC who have not previously received chemotherapy. According to data presented at ASCO, the combination therapy is superior to chemotherapy alone.
The addition of atezolizumab to bevacizumab plus carboplatin and paclitaxel improved the median progression-free survival (PFS) to 8.3 months with combination therapy versus 6.8 months with chemotherapy alone in wild-type paitents (HR, 0.62; 95% CI, 0.52-0.74;P<.001).4PFS improvements with added atezolizumab were also reflected in patients withEGFRorALKgenetic alterations, low or negative PD-L1 expression, and in those with liver metastases.
The rate of any-grade AEs was similar between the 2 arms (94.4% with added atezolizumab vs 95.4% with bevacizumab and chemotherapy). Treatment-related deaths occurred in 2.8% and 2.3% of patients in each arm, respectively. The most common immune-related AEs with added atezolizumab were rash (any-grade, 28.8%; grade 3/4, 2.3%), hepatitis/laboratory abnormalities (any-grade, 12.0%; grade 3/4, 4.1%), and hypothyroidism (any-grade, 12.7%; grade 3/4, 0.3%).
IMpower150 is still in progress, and the combination regimen used in the study is not currently approved by the FDA, although a supplemental biologics license application (sBLA) for this combination is being reviewed by the FDA for the treatment of patients with nonsquamous NSCLC. “It’s not yet completely clear how much the bevacizumab adds, and which patients get the most benefit from that,” Byers added.
The phase III CheckMate 227 compared the use of nivolumab plus ipilimumab (Yervoy) with standard chemotherapy to treat chemotherapy-naïve patients with stage IV or recurrent NSCLC with a tumor mutational burden (TMB) of at least 10 mutations per megabase. The 1-year PFS was 42.6% with the immunotherapy combination versus 13.2% with chemotherapy; median PFS was 7.2 months (95% CI, 5.5-13.2) in the combination group and 5.5 months (95% CI, 4.4-5.8) in the chemotherapy group (HR, 0.58; 97.5% CI, 0.41-0.81;P<.001).5The OS data have not yet been released.
Updated results presented at the ASCO meeting showed that the immunotherapy doublet also demonstrated superiority to the combination of nivolumab plus chemotherapy.6In patients with high TMB and PD-L1 expression below 1%, the median PFS was 7.7 months in the nivolumab/ipilimumab group, 6.2 months with nivolumab/chemotherapy, and 5.3 months with chemotherapy alone.
AEs were reduced with nivolumab/ipilimumab (any-grade, 74%, grade 3/4, 25%) compared with both nivolumab/chemotherapy (any-grade, 92%, grade 3/4, 52%) and chemotherapy alone (any-grade, 77%, grade 3/4, 35%).
CheckMate 568, a single-arm phase II study, is attempting to determine whether TMB can serve as a biomarker for likely clinical benefit from dual immune checkpoint blockade with nivolumab and ipilimumab in the frontline setting. “The question is, can we identify which patients are going to most likely benefit from immunotherapy or immunotherapy combinations with other targeted agents or chemotherapy?” questioned Minetta Liu, MD, research chair for the Department of Oncology at Mayo Clinic.
To date, the study data have demonstrated that a TMB of at least 10 mutations per megabase is associated with an enhanced response, regardless of PD-L1 expression, with objective response rates (ORRs) of greater than 40%. ORRs were 9%, 15%, 44%, and 39% in patients with a TMB <5, <10, ≥10, and ≥15 mutations per megabase, respectively.7
Cohort G of the phase II KEYNOTE-021 trial examined patients with previously untreated stage IIIb/IV nonsquamous NSCLC withoutEGFRmutations orALKtranslocations. Patients received carboplatin/pemetrexed followed by pembrolizumab and pemetrexed maintenance therapy or carboplatin/pemetrexed followed by pemetrexed maintenance therapy. At 12 months, patients who received the immunotherapy/chemotherapy combination had a PFS of 56% versus 34% for those who received chemotherapy alone. OS at 24 months was also improved (67% vs 48%, respectively). The median OS was still not reached in the pembrolizumab/chemotherapy arm after longer follow-up compared with 21.1 months in the chemotherapy alone arm (HR, 0.56; 95% CI, 0.32-0.95;P= .01508).8
The phase III KEYNOTE-189 trial was the confirmatory trial for the phase II KEYNOTE-021 data. KEYNOTE-189 compared the use of pembrolizumab plus pemetrexed and platinum-based chemotherapy with chemotherapy alone in patients with previously untreated stage IV nonsquamous NSCLC and noEGFRorALKalterations. Median PFS was 8.8 months (95% CI, 7.6-9.2) with immunotherapy/chemotherapy and 4.9 months with chemotherapy alone. The ORR was also higher with combination therapy compared with chemotherapy (47.6% vs 18.9%, respectively).9
The FDA granted a priority review for an sBLA for frontline pembrolizumab in combination with chemotherapy as a treatment for patients with metastatic nonsquamous NSCLC based on the results of this trial.
According to a press release from Roche, the manufacturer of atezolizumab, the phase III IMpower130 trial reached its co-primary endpoints for OS and PFS and demonstrated that atezolizumab plus carboplatin and nab-paclitaxel (Abraxane) chemotherapy prolonged survival in patients with advanced nonsquamous NSCLC.10Data from the trial are expected to be presented at an upcoming conference.
Squamous NSCLC
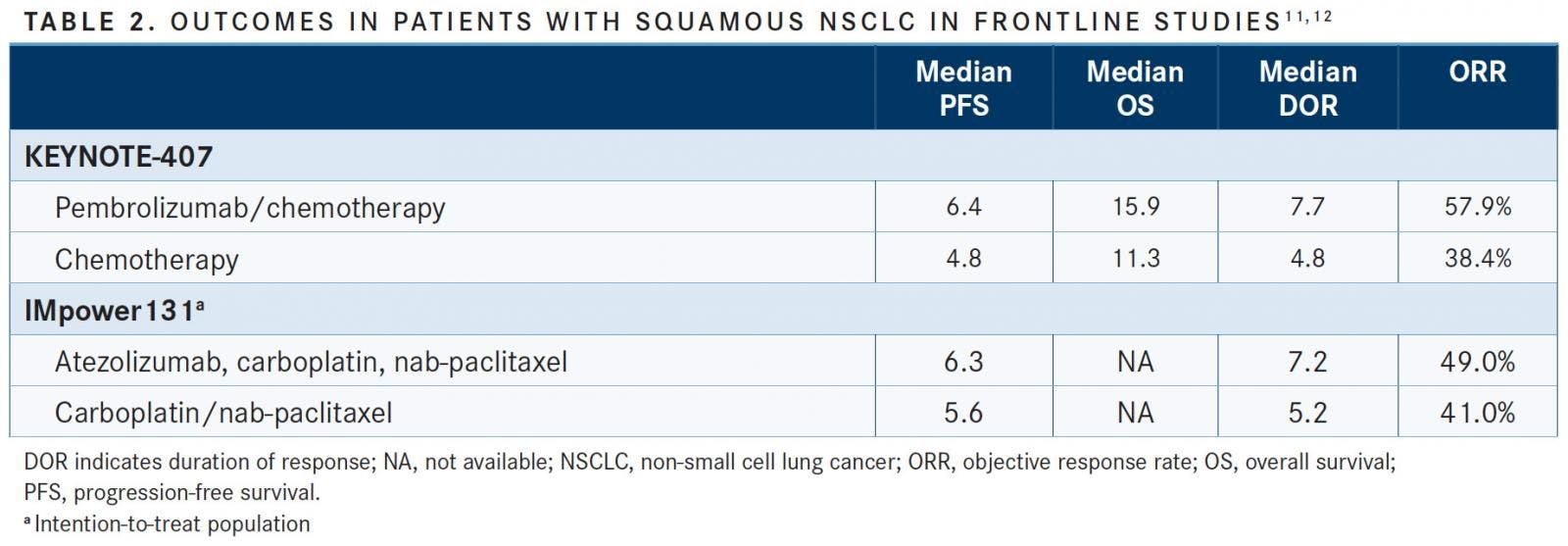
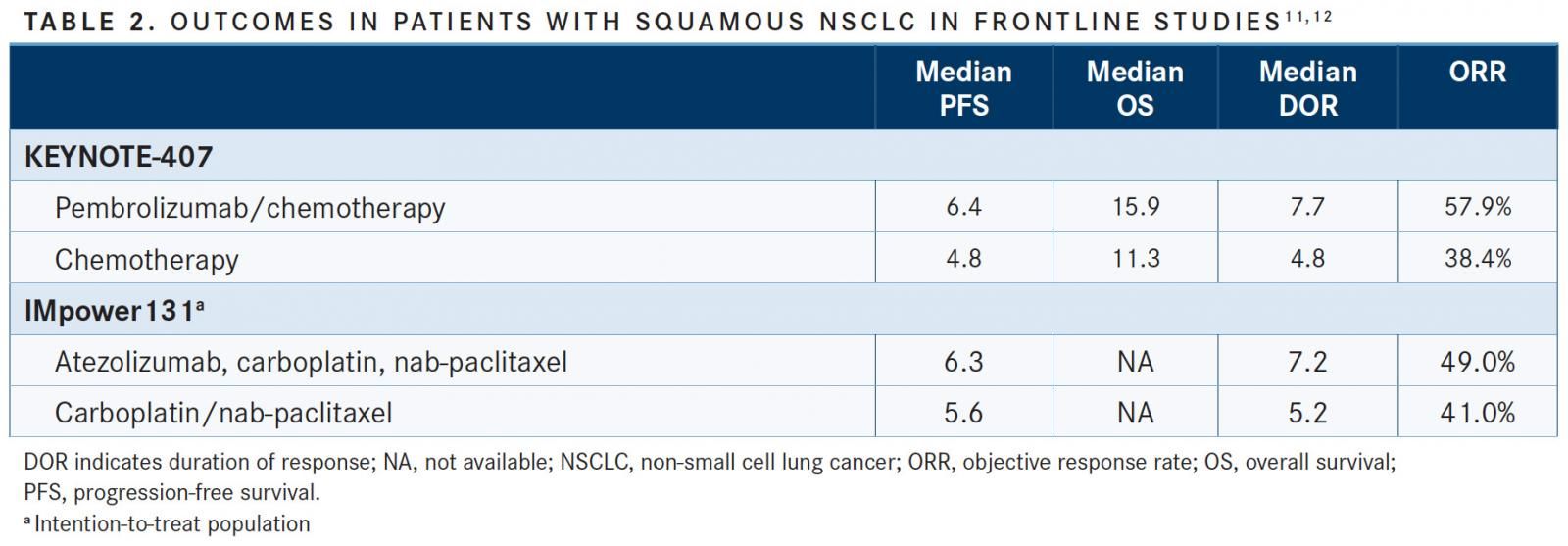
“Up until June of this year, if you had newly diagnosed lung cancer and your histology was squamous cell carcinoma, you needed to have more than 50% PD-L1 expression to get immunotherapy. If you had less than 50%, the standard of care was chemotherapy alone,” Molina explained. Two large phase III trials have shifted that standard of care (TABLE 2).
In the phase III KEYNOTE-407 trial, 560 untreated patients with metastatic squamous cell NSCLC were randomized to receive carboplatin 6 mg/mL/min and paclitaxel 200 mg/m2 every 3 weeks or nab-paclitaxel 100 mg/m2 weekly plus pembrolizumab or saline placebo for 4 cycles followed by pembrolizumab/placebo for a total of 35 treatments.11Patients who received the immunotherapy/chemotherapy combination had an ORR of 57.9% versus 38.4% in those who received chemotherapy alone. The median OS was 15.9 months with the combination compared with 11.3 months with chemotherapy (HR, 0.64; 95% CI, 0.49-0.85;P= .0008). OS benefits were observed regardless of PD-L1 level, age, gender, and performance status.

Additionally, AEs were less common in the combination cohort. The incidence of grade ≥3 AEs was 64.4% for combination therapy and 74.5% for chemotherapy alone. “Even patients with low PD-L1 expression tend to do better on this combination regimen,” stated Molina.
In May 2018, an sBLA was submitted to the FDA for the combination of pembrolizumab and chemotherapy for the treatment of patients with advanced squamous cell carcinoma. According to Molina, “The rumor out there is that this combination is going to be approved by October. It’s already working its way into the standard of care.”
The SITC consensus guidelines state that “the Task Force decided to prospectively consider combination pembrolizumab plus chemotherapy as an option for the treatment of patients with advanced squamous cell NCSLC and supports its use in appropriate patient subgroups if and when FDA approval is official.”1
The IMpower131 phase III trial investigated the addition of atezolizumab to carboplatin and paclitaxel or nab-paclitaxel as first-line treatment for patients with advanced squamous NSCLC. The group of patients that received atezolizumab plus carboplatin and nab-paclitaxel experienced a longer median PFS compared with those who received chemotherapy alone (6.3 vs 5.6 months, respectively; HR, 0.71; 95% CI, 0.60-0.85;P= .0001). Moreover, the PFS rate at 12 months was double with combination therapy (24.7% vs 12.0%, respectively).12PFS benefits were observed across all PD-L1 subgroups. Common immune-related AEs in the atezolizumab arm included rash, hepatitis, hypothyroidism, and pneumonitis.
Incorporating Trial Data Into Clinical Practice and Remaining Questions
“The nice thing, in terms of trying to keep up with rapidly changing treatment approaches, is that it’s not very complicated,” Byers suggested. “The data so far suggest that, essentially, all patients with NSCLC, with very few exceptions, have the potential to benefit from the addition of immunotherapy.”
Testing for PD-L1 expression has now become a standard of care; “at this point, it should be done in anyone who is diagnosed with NSCLC,” according to Liu. She and others are working to refine biomarker testing in an effort to further improve care. “If you read the fine print, each checkpoint inhibitor has a different assay for PD-L1 testing which was developed in conjunction with the medication,” Liu said. “But as a clinician, we don’t want to order PD-L1 testing multiple different ways. We’re trying to figure out if we can standardize an assay so that a patient who is diagnosed with NSCLC can have 1 assay done, and that leads to the ability to prescribe nivolumab, pembrolizumab, atezolizumab, and others.”
Liu and others are also working to develop biomarker tests that clinicians can use to monitor and adjust immunotherapy. “We know that there are patients who benefit from immunotherapy for a while, but then it stops working,” she said. Radiographic monitoring is not ideal, as pseudoprogression is a positive finding in the setting of immunotherapy. According to Liu, “We’re hoping to develop tools [that] clinicians can use to better determine who is benefiting from immunotherapy, and at what point we need to switch therapy.”
Now that the benefits of immunotherapy have placed it as a frontline therapy for advanced NSCLC, some investigators are studying the effectiveness of immunotherapy prior to surgical intervention,13 including the ongoing phase III trial of neoadjuvant nivolumab/ipilimumab versus nivolumab/chemotherapy or chemotherapy alone in patients with stage Ib-IIIa NSCLC (NCT02998528). “We don’t have a lot of data on that yet,” Byers said. “What has been seen so far is striking in terms of the potential responses, and the effects immunotherapy may have [in] the earliest-stage patients as well.”
References:
- Brahmer JR, Govindan R, Anders RA, et al. The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of non-small cell lung cancer (NSCLC).J Immunother Cancer.2018;6(1):75. doi: 10.1186/ s40425-018-0382-2.
- Reck M, Rodríguez-Abreu D, Robinson AG, et al; KEYNOTE-024 Investigators. Pembrolizumab versus chemotherapy for PD-L1positive non–small-cell lung cancer.N Engl J Med.2016;375(19):1823-1833. doi: 10.1056/NEJMoa1606774.
- Lopes G, Wu Y-L, Kudaba I, et al. Pembrolizumab versus platinum-based chemotherapy as first-line therapy for advanced/metastatic NSCLC with a PD-L1 TPS ≥ 1%: open-label, phase 3 KEYNOTE-042 study.J Clin Oncol.2018;36(suppl; abstr LBA4). meetinglibrary.asco.org/record/165950/abstract.
- Socinski MA, Jotte RM, Cappuzzo F, et al; IMpower150 Study Group. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC.N Engl J Med.2018;378(24):2288-2301. doi: 10.1056/NEJMoa1716948.
- Hellmann MD, Ciuleanu TE, Pluzanski A, et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden.N Engl J Med.2018;378(22):2093- 2104. doi: 10.1056/NEJMoa1801946.
- Borghaei H, Hellmann MD, Paz-Ares LG, et al. Nivolumab (nivo) + platinum-dou¬blet chemotherapy (chemo) vs chemo as first-line (1L) treatment (tx) for advanced non-small cell lung cancer (NSCLC) with <1% tumor PD-L1 expression: results from CheckMate 227.J Clin Oncol.2018;36(suppl; abstr 9001). meetinglibrary.asco.org/ record/160783/abstract.
- Ramalingam SS, Hellmann MD, Awad MM, et al. Tumor mutational burden (TMB) as a biomarker for clinical benefit from dual immune checkpoint blockade with nivolumab (nivo) + ipilimumab(ipi) in first-line (1L) non-small cell lung cancer (NSCLC): identification of TMB cutoff from CheckMate 568. Presented at: 2018 AACR Annual Meeting; April 14-18, 2018; Chicago, IL. Abstract CT078.
- Gentzler RD, Langer CJ, Borghaei H, et al. 24-month overall survival from KEYNOTE-021 cohort G: Pemetrexed-carboplatin plus pembrolizumab as first-line therapy for advanced nonsquamous NSCLC.J Clin Oncol.2018;36(suppl; abstr 9026). meetinglibrary.asco.org/record/160335/abstract.
- Gandhi L, Rodgríguez-Abreu D, Gadgeel S, et al; KEYNOTE-189 Investigators. Pembrolizumab plus chemotherapy in metastatic nonsmall-cell lung cancer.N Engl J Med.2018;378(22):2078-2092. doi: 10.1056/NEJMoa1801005.
- Phase III IMpower130 study showed Roche’s Tecentriq (atezolizumab) plus chemotherapy (carboplatin and Abraxane) helped people with metastatic non-squamous NSCLC live significantly longer compared to chemotherapy alone [media release]. Roche website; May 29, 2018. www.roche.com/media/releases/med-cor-2018-05-29.htm. Accessed August 2, 2018.
- Paz-Ares L, Luft A, Tafreshi A. KEYNOTE-407: Phase 3 study of carboplatin-paclitaxel/nab-paclitaxel with or without pembrolizumab for metastatic squamous NSCLC.J Clin Oncol.2018;36(suppl; abstr 105). meetinglibrary.asco.org/record/161684/abstract.
- Jotte RM, Cappuzzo F, Vynnychenko I, et al. IMpower131: Primary PFS and safety analysis of a randomized phase III study of ateolizumab + carboplatin + paclitaxel or nab-paclitaxel vs carboplatin + nab-paclitaxel as 1L therapy in advanced squamous NSCLC.J Clin Oncol.2018;36(suppl; abstr LBA9000). meetinglibrary. asco.org/record/165951/abstract.
- Owen D, Chaft JE. Immunotherapy in surgically resectable non-small cell lung cancer.J Thorac Dis.2018;10(suppl 3):S404-S411. doi: 10.21037/jtd.2017.12.93.











Multiple Resistance Mechanisms Thwart Efficacy for Third-Generation TKIs in NSCLC
April 7th 2024An important clinical strategy that focuses on improved frontline EGFR TKI regimens may help combat acquired EGFR TKI resistance and further streamline treatment options in subsequent lines, according to Balazs Halmos, MD.
Read More

