Glioblastoma Expert Calls for Changes to Clinical Trial Design
Failed clinical trials in glioblastoma are hampering the path toward novel treatment regimens in this difficult-to-treat malignancy and old approaches to clinical trial design are reducing the appetite for involvement, according to Erik P. Sulman, MD, PhD.
Erik P. Sulman, MD, PhD
Failed clinical trials in glioblastoma (GBM) are hampering the path toward novel treatment regimens in this difficult-to-treat malignancy and old approaches to clinical trial design are reducing the appetite for involvement, according to Erik P. Sulman, MD, PhD.
Trials with negative results mean a lack of enthusiasm for the treatment of GBM, and many drug companies have chosen to leave the market as a result, said Sulman, professor and vice chair of research in the Department of Radiation Oncology and codirector of the Brain Tumor Center at the Laura and Isaac Perlmutter Cancer Center at NYU Langone Health in New York, New York. He delivered a presentation on the current clinical trial landscape atMedical Crossfire®: Overcoming Clinical Inertia in Glioblastoma Multiforme, hosted by Physicians’ Education Resource®, LLC, on October 22, 2018, in San Antonio, Texas.1
With less than 15% of patients with GBM enrolling in clinical trials, Sulman said it is important to maximize the efficiency of trial design for emerging technologies, namely tumor-treating fields (TTFs) and novel immuno- and molecular-oncology treatments.
Sulman pointed to areas that need to be addressed in developing a new clinical trial paradigm in GBM. They include the current provider bias that influences which clinical trials are performed; patient access, or lack thereof, to a center that provides the option to participate; costs to the patient; exclusion of emerging therapies and technologies in clinical trial design; and the fact that new agents often fail in the recurrent setting and are then abandoned.
For the latter, he used the example of the EF-11 trial comparing TTF with standard-of-care chemotherapy in patients with recurrent disease. Limitations of this study stemmed from the fact that more than 40% of patients were in their third disease recurrence, including those who had failed on bevacizumab (Avastin), and the TTFs failed to demonstrate superiority over “established” chemotherapy regimens.2
Fortunately, Sulman said, TTFs went on to gain approval from the FDA, but this may not have been the case with other treatments or technologies.
Treatment Delays Lead to Participant Withdrawals
Other barriers to participation may stem from treatment delays, especially those that result from prerandomization testing. Molecular testing is necessary for stratification in many GBM clinical trials, but patients and providers often become impatient and withdraw.
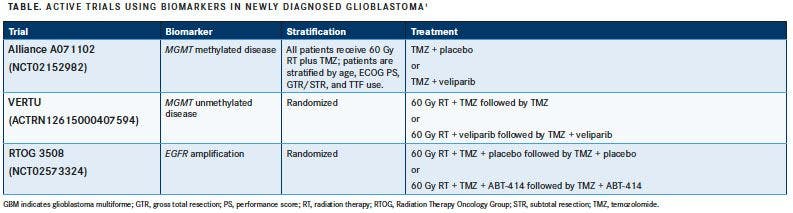
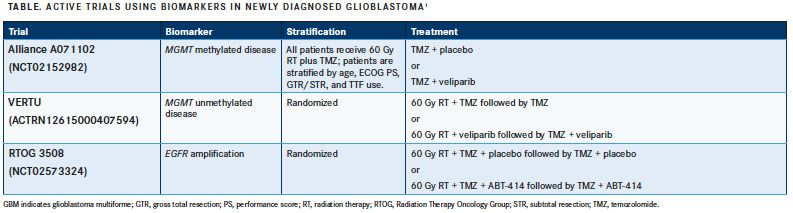
Many are concerned with the time between surgery and the start of radiation therapy. Sulman said that almost all clinical trials currently enrolling require this delay to complete proper testing, but this should never be a barrier to participation (TABLE).1He said that as providers, radiation oncologists need to assure their patients that waiting a few weeks for their test results is a safe option.
Sulman used the phase III Radiation Therapy Oncology Group (RTOG) trials 0525 and 0825 as examples, in whichMGMTgene expression was essential to the clinical trial stratification.3,4“We know that molecular testing up front prior to randomization is easily accomplished, and these trials recruited at rapid rates,” he said.
Results of several studies examining the relevance of radiotherapy timing and patient outcomes showed that waiting a few weeks after surgical resection did not have a negative impact on patient outcomes.5,6In fact, a retrospective analysis of 16 RTOG studies found that best outcomes were observed in patients who delayed radiotherapy treatment for 4 weeks or longer after surgery compared with patients who received treatment at varying intervals less than 4 weeks (P<.0001).7
Immuno-Oncology Treatment of GBM
Another factor to consider with the treatment of recurrent GBM is the effect temozolomide (Temodar) has on the immune microenvironment. According to Sulman, hypermutated tumors can result from temozolomide treatment and were shown to have more CD8-positive T cells and a different macrophage infiltrate profile than nonhypermutated tumors.8
“This suggests there is a potential advantage to having hypermutation in terms of the immune cell infiltrate. Indeed, this has led to how we think about immunotherapy trials,” Sulman said. “Temozolomide itself is causing this hypermutation to develop.”
He went on to add that only about 3% to 4% of tumors have hypermutation after treatment and even fewer present with it at initial diagnosis. But what about in the rest of the patient population?
Trials combining checkpoint inhibitors with radiotherapy for at least 1 component of the trial have yielded some negative results so far in the recurrent setting, Sulman said, but other trials are still ongoing. He suggested that negative results in these trials will continue to be observed because they are not all designed by the same standard. There is no prevailing guidance for timing of the drug, timing of radiation, and, more important, the radiation dose.
“Many of the trials are likely to be negative because these factors were not incorporated…, and as a result, we may throw the baby out with the bathwater,” he said.
Studies comparing stereotactic and fractionated radiation have produced conflicting results. This has left providers without guidance for deciding on a standardized optimal dose of radiation for use in conjunction with immunotherapy.
“There are so many variables to test. How do we test them all?” Sulman asked, adding that pressure on drug companies to launch clinical trials hinders their ability to try more permutations of radiation and drug dosage.
Novel Ways to Treat With Radiation
Sulman mentioned that finding new methods for GBM treatment requires clinicians to think back to their training and recall the 4R’s of radiation therapy: repair of cellular damage, reoxygenation of the tumor, redistribution within the cell cycle, and repopulation of cells.

Using these as a guide, he highlighted some novel targets. A phase I study of the radiosensitizing agent motexafin gadolinium (MGd) plus chemoradiotherapy with temozolomide showed tolerability in patients with GBM yet no significant improvements in overall survival.9In contrast, another study examining MGd plus whole-brain radiation therapy in patients with brain metastases improved time to neurologic progression in all patients, although not significantly, and improved neurocognitive function in patients with lung cancer.10
Results from preclinical studies have shown that MET promotes GBM stemlike cell radio resistance; therefore, MET inhibitors may affect DNA repair when paired with radiation therapy. However, results of these trials have yet to make an impact on the treatment landscape, Sulman said.11Similarly, attempts at decreasing hypoxia are being examined because of its negative impact on radio- and immunotherapy in cancer treatment.12
Layering Trials May Be the Future
Sulman wondered whether the current model of clinical trial design would work going forward in a difficult-to-treat disease like GBM. “These negative trials that keep happening reduce the appetite for involvement from industry,” he said, adding that a lukewarm attitude could cause drug companies to leave the market.
He said that rapid patient screening is key to overcoming many of the obstacles that currently hinder the treatment of GBM.
The INSIGhT trial consists of a single control arm and multiple experimental arms that patients are assigned to based on biomarker testing. Two of the experimental arms treat patients with radiotherapy and temozolomide plus either neratinib (Nerlynx), an EGFR, HER2, and HER4 inhibitor, or the CDK4/6 inhibitor abemaciclib (Verzenio). The other arm replaces temozolomide with CC-115, a TORC1/2 and DNA-PK inhibitor, in both the concurrent and adjuvant phases.13
“This is one approach, but it still relies on the standard evaluation of each arm over time,” Sulman said, “and this will still take a long time to test a number of agents.”
One of the most promising approaches that Sulman mentioned was the GBM AGILE novel multiarm platform trial.14 The 2-stage assessment uses a Bayesian analysis to identify effective therapies based on their impact on overall survival and then tests highly effective therapies using fixed randomization.
“You end up selecting for the treatments. The idea is you are feeding multiple treatments in here, and in general, you are not selecting the patients beyond [biomarker] groups,” said Sulman. “You are just putting them in the [trial], and if that agent ends up enriching [their outcomes], then that agent will graduate, and if…the Bayesian analysis shows there is no benefit for the next patient that is added, it will just disappear.”
He said this is the most rapid approach to screening because drug companies can seek registration once the agents or combinations graduate, and then they are automatically put into an expansion cohort.
References:
- Sulman E. Overcoming clinical inertia in GBM: clinical trials and therapeutic applications. Presented at: Medical Crossfire®: Overcoming Clinical Inertia in Glioblastoma Multiforme: the Experts Weigh In on Recent Data Sets and Next Steps to Move the Field Forward; October 22, 2018; San Antonio, TX.
- Hottinger AF, Pacheco P, Stupp R. Tumor treating fields: a novel treatment modality and its use in brain tumors. Neuro Oncol. 2016;18(10):1338-1349. doi: 10.1093/neuonc/now182.
- RTOG 0525 protocol information. Radiation Therapy Oncology Group website. rtog.org/ClinicalTrials/ProtocolTable/StudyDetails.aspx?study=0525. Updated December 15, 2016. Accessed November 10, 2018.
- RTOG 0825 protocol information. Radiation Therapy Oncology Group website. rtog.org/clinicaltrials/protocoltable/studydetails.aspx?study=0825. Updated June 30, 2017. Accessed November 10, 2018.
- Wehming FM, Wiese B, Nakamura M, Bremer M, Karstens JH, Meyer A. Malignant glioma grade 3 and 4: how relevant is timing or radiotherapy? Clin Neurol Neurosurg. 2012;114(6):617-621. doi: 10.1016/j.clineuro.2011.12.024.
- Lai R, Hershman DL, Doan T, Neugut AI. The timing of cranial radiation in elderly patients with newly diagnosed glioblastoma multiforme. Neuro Oncol. 2010;12(2):190-198. doi: 10.1093/neuonc/nop004.
- Blumenthal DT, Minhee W, Mehta MP et al. Short delay in initiation of radiotherapy may not affect outcomes of patients with glioblastoma: a secondary analysis from the radiation therapy oncology group. J Clin Oncol. 2009;27(5):733-739. doi: 10.1200/JCO.2008.18.9035.
- Wang Q, Hu B, Hu X, et al. Tumor evolution of glioma intrinsic gene expression subtype associates with immunological changes in the microenvironment. Cancer Cell. 2017;32(1):42-56.e6. doi: 10.1016/j.ccell.2017.06.003.
- Brachman DG, Pugh SL, Ashby LS, et al. Phase 1/2 trials of temozolomide, motexafin gadolinium, and 60-Gy fractionated radiation for newly diagnosed supratentorial glioblastoma multiforme: final results of RTOG 0513. Int J Radiat Oncol Biol Phys. 2015;91(5):961-967. doi: 10.1016/j.ijrobp.2014.12.050.
- Mehta MP, Rodrigus P, Terhaard CH, et al. Survival and neurologic outcomes in a randomized trial of motexafin gadolinium and whole-brain radiation therapy in brain metastases. J Clin Oncol. 2003;21(13):2529-2536. doi: 10.1200/JCO.2003.12.122.
- De Bacco, D’Ambrosio A, Casanova E, et al. MET inhibition overcomes radiation resistance of glioblastoma stem-like cells. EMBO Mol Med. 2016;8(5): 550-568. doi: 10.15252/emmm.201505890.
- Graham K, Unger E. Overcoming tumor hypoxia as a barrier to radiotherapy, chemotherapy and immunotherapy in cancer treatment. Int J Nanomedicine. 2018;13:6049-6058. doi: 10.2147/IJN.S140462.
- Alexander BM, Trippa L, Gaffey SC, et al. Individualized screening trial of innovative glioblastoma therapy (INSIGhT). J Clin Oncol. 2017;35(suppl 15; abstr TPS2079). doi: 10.1200/JCO.2017.35.15_suppl.TPS2079.
- Alexander BM, Ba S, Berger MS, et al; GBM AGILE Network. Adaptive global innovative learning environment for glioblastoma: GBM AGILE. Clin Cancer Res. 2018;24(4):737-743. doi: 10.1158/1078-0432.CCR-17-0764.