Ongoing Data Support Frontline Triplet in NSCLC
Data from the phase 3 POSEIDON trial support the use of tremelimumab, durvalumab, and chemotherapy for patients with metastatic non–small cell lung cancer, including harder-to-treat subgroups, in the first-line.


Updated findings from the phase 3 POSEIDON trial (NCT03164616) support the use of tremelimumab (Imjudo), durvalumab (Darzalex), and chemotherapy as a first-line combination approach vs chemotherapy alone in patients with metastatic non–small cell lung cancer, including harder-to-treat subgroups. Results included analyses by nonsquamous or squamous histology, and by STK11, KEAP1, or KRAS mutational status for mutation-positive or wild type disease. The -year follow-up data were presented at the European Society for Medical Oncology (ESMO) Immuno-Oncology Congress 2023 by Solange Peters, MD, PhD.
“After a median follow-up of more than 5 years, [POSEIDON] demonstrated a durable long-term overall survival [OS] benefit [when] adding a limited course of tremelimumab and durvalumab,” said Peters, professor and chair of the Medical Oncology and Thoracic Malignancies Programme, Department of Oncology, University Hospital of Lausanne, Switzerland. “The 5-year [OS] rate [for the triplet] was more than twice as high than chemotherapy, 15.7% vs 6.8%,” Peters continued.
In POSEIDON, 1013 patients were randomly assigned to 3 arms: tremelimumab plus durvalumab plus chemotherapy (arm 1); durvalumab plus chemotherapy (arm 2); or chemotherapy alone arm (arm 3). The dosing schedule was every 3 weeks for 4 cycles, every 3 weeks for 4 cycles, and every 3 weeks for up 6 to cycles, respectively. Patients in arm 1 received tremelimumab at week 16 only and durvalumab every 4 weeks until disease progression. Patients in arm 2 received durvalumab every 4 weeks until disease progression.
Eligible patients had an ECOG performance status 0 or 1, had EGFR or ALK wild type, and were treatment naive for metastatic disease. “ Patients were stratified according to PD-L1 expression, disease stage, and histology,” Peters said. “Prespecified long-term follow-up end points included [OS] and serious adverse events [AEs],” she added.
Investigators noted that long-term OS benefit comparing the triplet combination vs chemotherapy alone showed a greater benefit in patients with nonsquamous histology with an HR of 0.69 and 5-year OS rates of 20.5% vs 9.1%.
In the mutation-evaluable population, 30% had a KRAS mutation (n = 37), 6% had a KEAP1 mutation (n = 37) , and had a STK11 mutation (n = 87).


The updated OS by STK11 mutation showed that patients treated with the triplet regimen had a median OS of 15.0 months (HR, 0.57; 95% CI, 0.32-1.04) compared with 6.9 months for patients treated with durvalumab and chemotherapy (HR, 1.02; 95% CI, 0.59-1.80) and 10.7 months with patients treated with chemotherapy only (95% CI, 6.0-14.9). The OS benefit was maintained for the triplet regimen in patients with STK11 mutation with an HR of 0.57 and 5-year OS rates of 12.9% vs 0% for the chemotherapy regimen.
The updated OS by KEAP1 mutation status across all histologies showed that the OS benefit was maintained for the triplet regimen with an HR of 0.43. In patients with the KEAP1 mutation, patients who were treated with the triplet had a median OS of 13.7 months (HR, 0.43; 95% CI, 0.16-1.25), patients treated with the doublet had a median OS of 8.1 months (HR, 0.77; 95% CI, 0.31-2.15), and patients treated with chemotherapy had a median OS of only 8.7 months.
In patients with KRAS mutations, the OS benefit maintained for the triplet regimen vs chemotherapy alone led to an OS of 0.55 and a 5-year OS rate of 21.7% vs 8.1%, respectively.
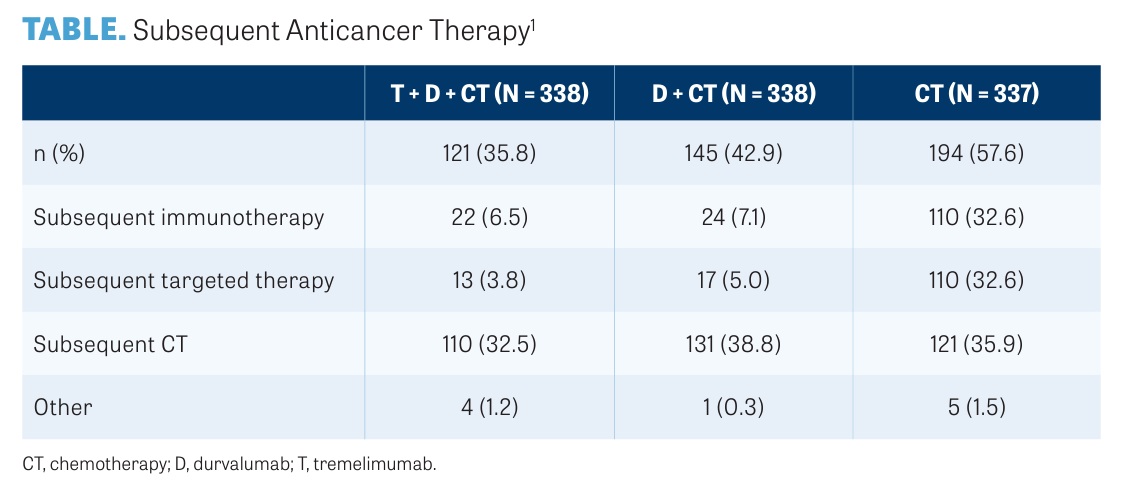
The TABLE1 shows subsequent systemic anticancer therapy by regimen arm. "In the chemotherapy alone arm, 63% of the patients received subsequent immunotherapy vs more or less [than] in the immunotherapy arms subsequently,” Peters said.
Serious adverse events (SAEs), including AEs leading to death, were collected during long-term follow-up. No other safety data were collected after the final analysis for OS superiority. Since the final analysis, 7 additional patients experienced SAEs (1 considered to be treatment related) and 4 additional patients had AEs leading to death (none were treatment related).
“Across patient subgroups, long-term OS benefit was generally consistent with the intention-to-treat population,” Peters said. “ Consistent with earlier analysis, the addition of tremelimumab to durvalumab and chemotherapy provided OS benefit regardless of PD-L1 expression,” concluded Peters.
REFERENCE
1. Peters S, Cho BC, Luft A, et al. Durvalumab (D) ± tremelimumab (T) + chemotherapy (CT) in fi rst-line metastatic (m) NSCLC: 5-year overall survival (OS) update from the POSEIDON study. Ann Oncol. 2023;20(suppl 1):100535. doi:10.1016/ iotech/iotech100535










Intracranial Response Data Supports Use of Brigatinib in ALK+ NSCLC
April 26th 2024During a Case-Based Roundtable® event, Yasir Y. Elamin, MD, discussed the intracranial efficacy of brigatinib from the ALTA-1L trial for patients with ALK+ non–small cell lung cancer in the first article of a 2-part series.
Read More


Marks Explores Cardiac Toxicities and Dosing Concerns of BTK Inhibitors in CLL
April 26th 2024During a Case-Based Roundtable® event, Stanley M. Marks, MD, moderated a discussion on the impact of cardiac adverse events on patients who receive a Bruton tyrosine kinase inhibitor for chronic lymphocytic leukemia.
Read More

Nogapendekin Alfa Plus Checkpoint Inhibition Improves Survival in NSCLC
April 25th 2024Following its recent FDA approval in non-muscle-invasive bladder cancer, nogapendekin alfa has also shown overall survival benefits in addition to checkpoint inhibitor therapy in patients with non-small cell lung cancer.
Read More

Advances in Subsequent Therapies Shake Up Sequencing of ccRCC Treatment
April 25th 2024With the approval of belzutifan and other newer data for treating patients with recurrent renal cell carcinoma, the state of subsequent therapies is advancing beyond the reuse of frontline options with impacts on duration of response and quality of life.
Read More

