Roundtable Roundup: Multiple Myeloma
In separate, live virtual events, Jonathan L. Kaufman, MD, and Morie A. Gertz, MD, MACP, discussed concerns about using chimeric antigen receptor T-cell therapy for a patient with relapsed/refractory multiple myeloma who is experiencing rapid disease progression.
CASE SUMMARY
Eight years ago, a 63-year-old man received a diagnosis of multiple myeloma (IgGκ). He lived in a rural community. Recently, he presented with penta-refractory disease progression after 4 prior lines of therapy that included autologous stem cell transplant, 2 proteasome inhibitors, 2 immunomodulatory drugs, and 1 anti-CD38 antibody. He had hypertension controlled with lisinopril. His ECOG performance status was 1.


Professor, Department of Hematology and Medical Oncology
Emory University School of Medicine
Medical Director and Section Chief, Ambulatory Infusion Centers
Winship Cancer Institute of Emory University
Atlanta, GA



Morie A. Gertz, MD, MACP
Hematologist/Oncologist
Chair, General Internal Medicine
Mayo Clinic
Rochester, MN

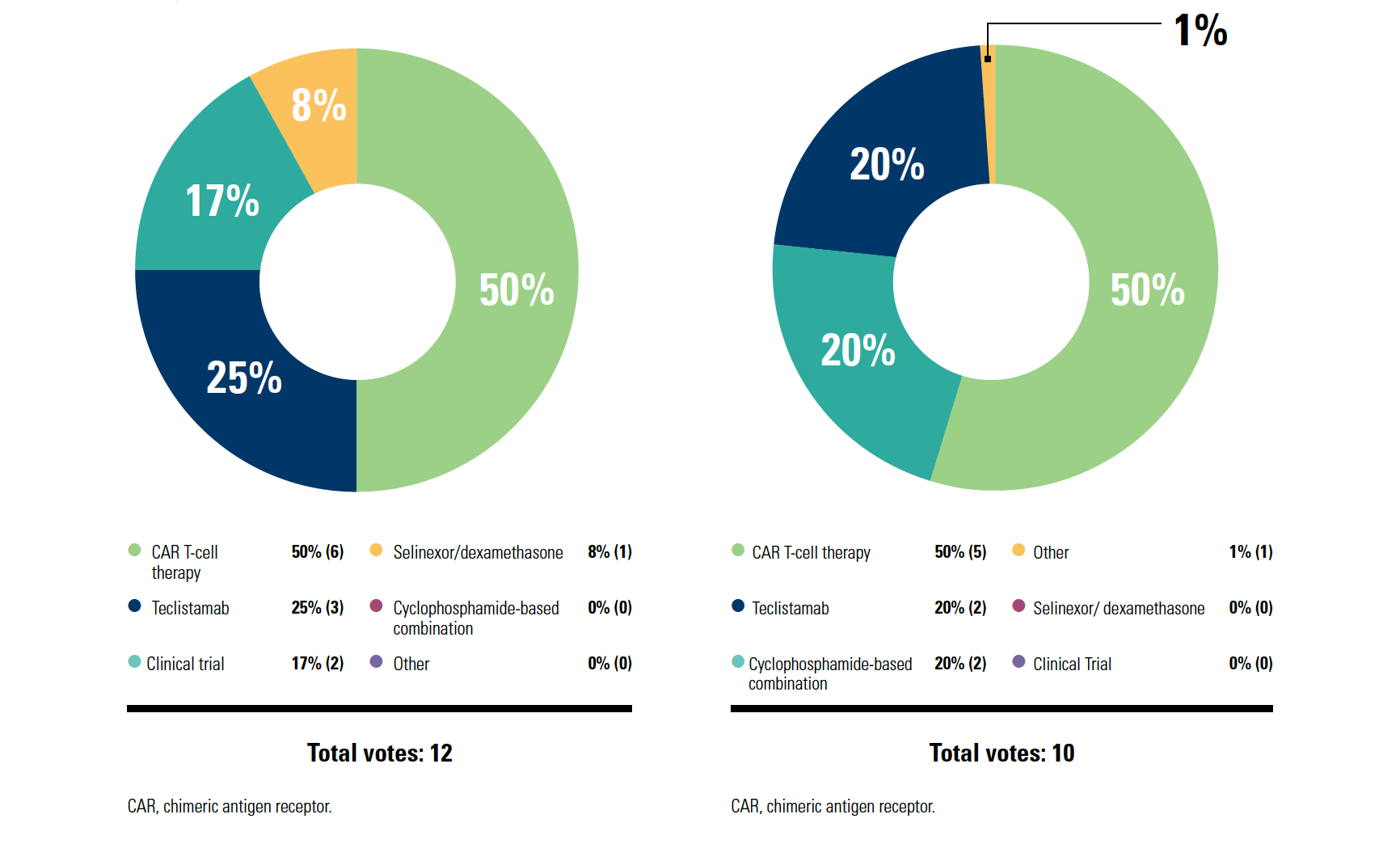
KAUFMAN: If I think about getting CAR T-cell therapy, if I think you as a patient need CAR T cells today, the best-case scenario is it happens in 3 or 4 months. That’s where we are today. [I hope] a year from now, we won’t be there…. It’s the logistics; although ideally maybe we like the efficacy, and we like the one-and-done nature of it—patients can come back to you and don’t have to have continuous therapy—it’s just not happening yet.
The way I think about it, for the patients with rapidly progressing disease, there’s no way that you can get lucky to have CAR T-cell therapy in [those] patients; you need bridging therapy. Then the more indolent relapse, where you see the relapse coming and you don’t stop therapy, that’s the patient who maybe can get a CAR T-cell slot 3 months from now.
Patient preference is important [for choosing next-line therapy]. When I talk to patients about it, some patients love the idea of one-and-done. Other patients don’t like how intense CAR T-cell therapy is and are OK with the ongoing therapy; they don’t like getting T cells collected, waiting the month, all those things. [Then there’s the] convenience logistics about getting it done—going to an academic center, getting the CAR T cells, coming back, and living a long, beautiful life. Performance status is critical. The way I lean is that [for patients with] better performance status, I can wait a bit and maybe that patient is right for CAR T cells.
GERTZ: Most CAR T-cell therapy mandates anywhere [state] that your [patient stays] 1 month at a medical center. So there’s no commute; they’re there, they get a hotel room, etc. CAR T-cell therapy would be a reasonable option, although for me, cyclophosphamide is a very common bridging therapy once they’re accepted.
Supply chain has limited access to commercial CAR T-cell therapy…it’s a real pain. Patients can sometimes wait months, and many of them don’t have months to wait. A significant cause of death is death on the waiting list, waiting to get availableCAR T-cell therapy.
The National Comprehensive Cancer Network guidelines [recommend] bendamustine, cyclophosphamide, or bendamustine combinations and then, [after 4 prior lines of therapy], CAR T cells, an antibody-drug conjugate, and the bispecific antibody teclistamab [Tecvayli]. You still have the option to use selinexor [Xpovio]. At this point, reimbursement hasn’t been a big problem, but it’s a hard drug to use.
















How Data Help Physicians Improve Operations and Achieve Health Equity
May 13th 2024A US health care executive survey found 30% see health equity solely as a social concern. Yet, it's about ensuring everyone has a fair shot at optimal health. Utilizing standardized data can shift care from reactive to preventive, easing strain on systems.
Read More


How BCMA CAR T-Cell Therapy Provides Later-Line Options in R/R Multiple Myeloma
May 10th 2024During a Case-Based Roundtable® event, Abdullah Khan, MBBS, discussed the different outcomes with idecabtagene vicleucel in patients with relapsed/refractory multiple myeloma in both the clinic and real-world settings in the second article of a 2-part series.
Read More

Landgren on MRD as an End Point for Multiple Myeloma Trials
May 1st 2024C. Ola Landgren, MD, PhD, discussed the FDA’s unanimous ODAC vote supporting minimal residual disease as an accelerated approval end point in multiple myeloma and the implications of this vote in the myeloma research field.
Read More

