Sequencing of CD19-Directed Therapy Is Still Up for Debate
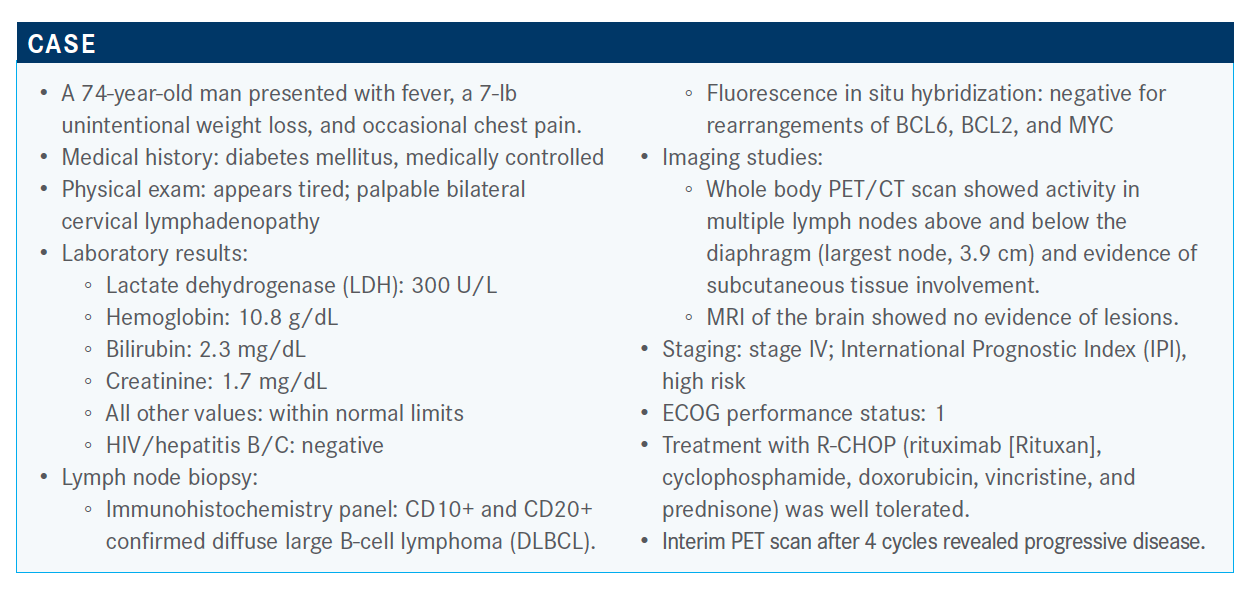
Gilles Salles, MD, PhD, discussed sequencing of CD-19 directed therapies for a 74-year-old patient with diffuse large B-cel lymphoma during a Targeted Oncology Case-Based Peer Perspective Roundtable event.


Gilles Salles, MD, PhD

Gilles Salles, MD, PhD, discussed sequencing of CD-19 directed therapies for a 74-year-old patient with diffuse large B-cell lymphoma (DLBCL) during a Targeted Oncology Case-Based Peer Perspective Roundtable event.


Targeted OncologyTM: What are the options for therapy?
SALLES: Options that are, right now, recommended by the NCCN [National Comprehensive Cancer Network] guidelines [include] GemOx [gemcitabine and oxaliplatin]. We also have polatuzumab vedotin [Polivy]/BR [bendamustine and rituximab], which is approved after 2 or more lines of therapy. There are a couple of other regimens that may or may not be useful.1 Tafasitamab [Monjuvi] has recently been introduced as a combination [with] lenalidomide [Revlimid].


Can you provide a brief overview of tafasitamab's mechanism of action and approved indications?
The approval for this combination was obtained in July, and the indication was for relapsed or refractory DLBCL not otherwise specified, including those arising from low-grade lymphoma [and in those] not eligible for autologous stem cell transplant.2
Tafasitamab, which [was also known as] MOR208, is an antibody directed against CD19. This antibody has been modified in its Fc portion in order to improve the immune mechanism of antibody-dependent cytotoxicity, antibody-dependent phagocytosis, and also direct cell death.
When used alone, tafasitamab has a limited activity. This was already published but based on some preclinical data and the experience with the efficacy of this drug, there was a rationale to combine it with lenalidomide. As we know, lenalidomide improves the activity of T and NK [natural killer] cells and can be used in this setting. Also, lenalidomide has been approved for mantle cell and follicular lymphoma in the relapse setting.
What data support the use of the tafasitamab combination in this setting?
The study that evaluated this combination is called L-MIND [NCT02399085], which used tafasitamab and lenalidomide. This was [in patients who were] relapsed or refractory, with 1 to 3 prior regimens of therapy, and in those not eligible for transplant, regardless of the reason.3
Patients received tafasitamab as an intravenous infusion at a fixed 12-mg/kg dose, and this was given weekly during the first 3 cycles and then every 2 weeks for the [remaining] cycles. During the first year of the study, lenalidomide was given at the usual dose of 25 mg per day, from days 1 to 21, with potential dose adaptation. I should mention, there is also a day 4 infusion of tafasitamab during the first cycle—quite a lot of infusions at the beginning, then infusion every 2 weeks. Patients who benefited from therapy—those who had stable disease, partial response [PR], or complete response [CR]—were able to continue the tafasitamab single agent without lenalidomide every 2 weeks until progression.
Please describe the inclusion criteria from this trial. What were the characteristics of this patient population?
The trial was open in several centers, and there was an aggressive attempt to recruit patients. The screening occurred progressively, and a substantial number of patients were not treated. A few patients were not treated because they progressed rapidly, but the majority were not treated because they didn’t fulfill the criteria for inclusion. In the majority of cases, these were biological criteria. The criteria [for exclusion] were rather standard, [such as] limited creatinine clearance, low platelet counts, or low performance status.
Patients who relapsed within 3 to 6 months after R-CHOP were eligible. [Later] the trial was modified, amended at the request of the health authority, to recruit patients who were not within this window of 6 months after R-CHOP.
There was an equilibrium between patients with a low IPI and high IPI; the majority of patients had advanced-stage disease, and 44% had elevated LDH. About half of the patients received only 1 prior line of therapy and so [some patients] were in the first relapse, whereas the others were treated later.
Because of modifications in the inclusion criteria during the trial, only a few patients had primary refractory disease, but patients could be refractory to their second line of therapy. There were a few patients who relapsed after stem cell transplant. Cell of origin was not well characterized.
What were the primary efficacy data from the L-MIND trial?
The primary end point for this study was the overall response rate, assessed by central review. The primary response showed 43% of the patients achieving a CR, 18% with PRs; more than 60% of the patients responded. A few patients had stable disease [14%] or progressive disease [16%] or were not evaluable [10%]. The majority of these responses were PET confirmed.
The most surprising, though impressive, result of these data was the fact that for the responding patients, we had a duration of response curve that tended to plateau after 6 to 9 months, having the majority of patients still remaining responsive. If we break this curve of duration of response by best response, it’s even more striking. The patients who had achieved only a PR [had a] failed response within a median of 4 months. For the patients who had achieved a CR, a significant number remained in response for more than 1.5 years.
The median PFS is about 1 year, or 12.1 months [95% CI, 5.7–not reached]. At 18 months, the PFS rate is 46%. The median [overall] survival was not reached and was at a rate of 75% at 12 months and 64% at 18 months.
When giving a CD19-directed therapy to a patient who potentially does not have CD19 expression, what concerns do you have?
Regarding CD19 expression at baseline in DLBCL, it’s extremely rare to have no expression in a patient who never received CD19-directed therapy. That’s clear when you want to give this drug or any CD19-directed therapy for this patient.
Then the question that comes up is whether we may eventually lose CD19 expression by using this drug and compromising the use of CD19-directed CAR [chimeric antigen receptor] T-cell therapy in the future. Or, vice versa, if we use CD19 CAR T-cell therapy, will we lose the opportunity to manage this regimen in the future?
Unfortunately, there are few data on that. We know that patients who were exposed to these drugs, which were patients with CLL [chronic lymphocytic leukemia], continued to express CD19.…I don’t think there have been demonstrations of the loss [of expression].
But there may be, still, some antibodies that may be coded to the antigen, preventing immediate CAR T-cell treatment. Having said that, when we use CAR T-cell therapy, we know that about one-third of the patients who relapse may lose CD19 [expression].
I think this is an interesting and important question. We have the answer yet.…How to sequence these agents remains unclear at this point. We have different options, and we may discuss with the patient which [CD19-directed therapy] we want to choose. Each has different availability, tolerability, and constraints.
What were the adverse effects (AEs) observed with the tafasitamab regimen in the L-MIND study for these patients?
The most common AEs were, essentially, hematologic. About half, or almost half, of the patients experienced grade 3/4 neutropenia. Only a few patients experienced febrile neutropenia that resolved rather quickly. Also, 15% of the patients had grade 3/4 thrombocytopenia.
There are clearly some hematologic toxicities, and what was found is that these essentially appeared during the first year of the study, when the combination of lenalidomide and tafasitamab [was used], leading t0, eventually, an adjusted dose of lenalidomide. Anemia was rare. Except for rashes, hypokalemia, and a few urinary infections, there were few grades 3/4 infections.
Essentially, hematologic toxicities of grade 3/4 were quite manageable, and a few of the AEs of grade 1/2 were reminiscent of the AEs that we found when we use lenalidomide.
There were a couple of serious AEs, as expected, in the population of relapse/refractory DLBCL. What I think is important is that only a few were suspected to be treatment related. Just 12% of the patients had to discontinue the combination therapy due to AEs. There were a few AEs of special interest. I should say that it was, essentially, allergic dermatitis, 2 or 3 cases of tumor flare of grade 1 to 3, and 1 patient who had a basal carcinoma. Infusion-related reactions were well prevented by the administration of steroids and other drugs. There were 4 deaths in the study that appear not be related to the study treatment.
If you use tafasitamab and lenalidomide, would it be hard later to collect the T cells for CAR T with this regimen?
No, I don’t think we have any issue of collecting T cells after lenalidomide or after tafasitamab. The question, again, is whether CD19 will be still expressed. At the present time, we assume that, yes, but they probably need wash out [time] between the last tafasitamab infusion and the administration of CAR T-cell therapy, which may eventually cover the time of CAR T-cell manufacturing. We have a case at Memorial Sloan Kettering Cancer Center where we did a biopsy a few days after the infusion and couldn’t detect CD19; this was probably by antigen masking. But when we performed subsequent biopsies after, I think, 3 to 4 weeks, we again found the antigen. This is just 1 case. There are other cases, and we need to see that.
Would you use this regimen in all patients in this setting?
I’m convinced that this is not the appropriate or the best choice regimen for a young patient [who is] fit and may eventually go for transplant. This raises the question [about] patients you bring for CAR T-cell therapy: Who are the patients in which you try that? We don’t know whether it can compromise CAR T-cell therapy or not. In the relapse setting, we already know that after CAR T-cell therapy, one-third of the patients may not be able to receive this regimen because of the loss of CD19.
We have to keep in mind that the median age of our patients with DLBCL is around 70 years. Not all patients go for CAR T-cell therapy. When taking care of elderly patients at our center for transplant, we’ll assess them carefully for eligibility for this intensive regimen. Obviously, we’ll have progress with the management of CAR T-cell therapy administration, but it’s a bit difficult at this time to say where, exactly, to position it.
I have to be a bit more cautious regarding this patient in particular, because this is a patient who had primary refractory disease. If we look in detail at the trial, there were few patients like that. They seem to respond, but we have a limited experience. It’s a good regimen for patients who relapse after 6 months or 1 year or had failed a second-line chemotherapy and [need] an alternative. But for the patients who are primary refractory, I will be personally encouraged to see more data in this setting before really moving it up front.
Are any other agents besides lenalidomide being explored as a partner for tafasitamab?
We have a trial called B-MIND [NCT02763319] that is presently almost completed and will look at BR versus bendamustine/tafasitamab in the relapse DLBCL setting. We know that the trial is not futile because it has been expanded, but I don’t know when we’ll see the results.
Regarding the optimal partner, the use of lenalidomide is potentiating the immune mechanism of action. We can take advantage of adding another compound, rituximab, because we don’t know if a triple combination will be more efficient versus a basic cytotoxic agent.
References:
1. NCCN. Clinical Practice Guidelines in Oncology. B-cell lymphomas, version 4.2020. Accessed December 1, 2020. https://bit.ly/35H3YW0
2. FDA grants accelerated approval to tafasitamab-cxix for diffuse large B-cell lymphoma. FDA. Updated August 3, 2020. Accessed December 1, 2020. https://bit.ly/34Emq2z
3. Salles G, Duell J, Gonz.lez Barca E, et al. Tafasitamab plus lenalidomide in relapsed or refractory diffuse large B-cell lymphoma (L-MIND): a multicentre, prospective, single-arm, phase 2 study. Lancet Oncol. 2020;21(7):978-988. doi:10.1016/ S1470-2045(20)30225-4
















Bispecific Antibodies and ADCs Deliver a Futuristic Horizon Across Lung Cancer Settings
October 23rd 2024Recent advancements in protein engineering, especially antibody-drug conjugates, show promise in lung cancer treatment, with ivonescimab outperforming pembrolizumab in PD-L1-positive advanced non-small cell lung cancer.
Read More


