
|Videos|September 25, 2018
Case 2: MRD Negativity in High-Risk Myeloma
Advertisement
Episodes in this series













EXPERT PERSPECTIVE VIRTUAL TUMOR BOARD
Ajai Chari, MD:You alluded to and did a great job presenting the data on the overall survival with the maintenance study. In the forest plot that you showedthe curve—the study that’s pulling it to the right is actually the IFM study, which is kind of what we saw. Why is it that on this side of the Atlantic we see an overall survival benefit and on the other side we don’t? When studies are designed, if the primary endpoint is progression-free survival, we have to remember that overall survival is an exploratory endpoint and can be confounded by salvage therapy.
In 2005, when the IFM study was done, if you got lenalidomide maintenance and you progressed, 50% of patients in that study who progressed went on to get more IMiD [immunomodulatory drug] therapy, which doesn’t make sense. If you are refractory to lenalidomide maintenance and you get more IMiD therapypossibly thalidomide, which is an inferior IMiD—is it surprising that you may lose the overall survival benefit that you gained from the maintenance? Whereas, in the United States, there was more appropriate salvage therapy with the PI [proteasome inhibitor]. Again, I’m kind of a stats nerd. I guess I find this interesting, but it’s really important. When we look at overall survival, if that was not a predefined endpoint and you’re not controlling for salvage lines of therapy, you really cannot speak definitively about the impact of your intervention for long-term sequalae.
C. Ola Landgren, MD, PhD:I think that was a very valid comment. It kind of speaks to the fact that we always have to go into the details of the data and not overinterpret them. When we pool data, there will be a lot of nuances. If we go and look through the duration of the therapy, there was also a big difference.
Ajai Chari, MD:Absolutely.
Nina Shah, MD:Yes, a huge difference.
C. Ola Landgren, MD, PhD:When they presented the data at the ASH Annual Meeting in 2009, they had found 7 cases of secondary malignancy. That triggered alarm throughout the French group, so they stopped the lenalidomide maintenance after a median duration of about 2 years. The American study kept on going. When the investigation was completed, the conclusion was that it provided more benefit than risk, so the American study kept on going.
Ajai Chari, MD:As confirmed by an overall survival benefit.
Nina Shah, MD:Right.
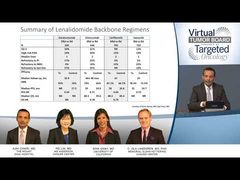
C. Ola Landgren, MD, PhD:That’s where you have the difference in overall survival. Maybe it’s also the duration of the maintenance? There was also a dosing difference. The CALGB study allowed for a dose of up to 15 mg, whereas the French study was dosed at 10 mg. We don’t know if that is contributing or not, but that’s another nuanced difference between the 2 studies.
Nina Shah, MD:Right. There was a presentation at the ASCO [American Society of Clinical Oncology] Annual Meeting this past year that suggested that higher lenalidomide maintenance was better, although it was a smaller study. And so, maybe even the 5-mg difference made a difference?
Ajai Chari, MD:Again, it’s great to have options for patients. Lenalidomide maintenance has the most robust data, as you’ve beautifully shown, but we recently heard that ixazomib maintenance showed a superior progression-free survival benefit. For patients, particularly those who have the t(4;14) translocation, a PI oral drug may be a better choice. Emory has also presented a combination of a PI and IMiD, and there’s also daratumumab in the maintenance setting.
Nina Shah, MD:Yes, and now there will be data with the GRIFFIN trial. I just want to bring this point up. Now you have big data. You have this meta-analysis. It doesn’t get better than randomized controlled trials and all of that, but we have smaller studies. And so, if this person was with you, should the patient receive maintenance therapy? A lot of us say OK. But then, what would you do? Would you just say “I have the most data with lenalidomide and you’re going to get lenalidomide,” or do you take these smaller studies into consideration? What would you do?
Ajai Chari, MD:I might actually offer this patient ixazomib because of the t(4;14) translocation. Historically, lenalidomide has improved but not overcome high-risk features. The inconvenience of giving other parenteral proteasome inhibitors makes ixazomib another choice. But, again, I think we have to also think about the patient tolerability and issues like neuropathy versus thrombotic events, myelosuppression, and diarrhea. Each drug has its own unique profile. The other point I would say is that I always tell patients that maintenance should be mindless. If you’re miserable on maintenance, I think we’re defeating the purpose. I want my patients to live longer and better, not just live longer with misery.
Nina Shah, MD:I’m so glad that you brought that up. We now have more studies incorporating patient-reported outcomes and quality of life analyses. That is so critical, especially in this age group where people have long-term treatment and need to know if they are going to be able to make it to family events. Can they work? As I say, age 70 is the new age 60. You want people to be very functional.
What about you, Ola? Would you give this patient maintenance? If so, what would you offer, given the details of the case?
C. Ola Landgren, MD, PhD:I would have a conversation with the patient and say that the standard of care in the United States would be to consider maintenance. I would say that there’s a meta-analysis showing that there is an overall survival benefit and that 1 of the 3 large studies really showed overall survival. The others didn’t. So, that’s kind of what the data are. I’d say for sure that there is a progression-free survival benefit. So, in that light, if the patient is interested in taking a pill for 3 out of 4 weeks, with the main target being to prolong progression, that would be a justifiable thing to do. Most of my patients would do that. I would offer them lenalidomide. I think ixazomib is a valid option. If you look at the NCCN [National Comprehensive Cancer Network] guidelines, they suggest that you can use Velcade [bortezomib] every other week. You can also use ixazomib as a single drug. Lenalidomide, for sure, has the longest track record, or more studies with more patients. That’s why we have progression-free survival and overall survival data. Just for the discussion here, I think it’s important to emphasize that there is no randomized study, at this point, that has compared lenalidomide to ixazomib, or lenalidomide to Velcade, proving superiority or inferiority. We don’t have that information. It’s a judgment call.
Transcript edited for clarity.
Advertisement
Related Content
Advertisement

































Advertisement
Advertisement
Trending on Targeted Oncology - Immunotherapy, Biomarkers, and Cancer Pathways
1
ASCO 2026 GU Cancer Highlights: Beyond the LBAs
2
Dr Tolaney on SG + Pembrolizumab Biomarker Data in First-Line mTNBC
3
FDA Approves Generic Eribulin Mesylate for Metastatic Breast Cancer
4
Bispecific ADC Iza-Bren Extends Survival in Advanced TNBC
5