
|Videos|September 25, 2018
Case 4: BCMA-Targeted CAR T-Cell Therapy in Myeloma
Advertisement
Episodes in this series








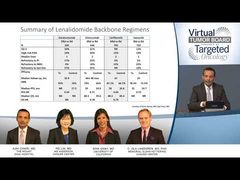





EXPERT PERSPECTIVE VIRTUAL TUMOR BOARDC. Ola Landgren, MD, PhD:Would you use any of the phase III combinations that have been published over the past 2 years in theNew England Journal of Medicineelotuzumab/Revlimid [lenalidomide]/dexamethasone, ixazomib/Revlimid/dexamethasone, carfilzomib/Revlimid/dexamethasone, or daratumumab/Revlimid/dexamethasone? Is there a good combination for a patient like this?
Nina Shah, MD:It’s really hard to say. Based on what we were talking about before, about how these trials were done, they were all done in Revlimid-sensitive patientsmany of them. This patient is not Revlimid sensitive. He has already had carfilzomib/lenalidomide/dexamethasone. He’s had daratumumab/pomalidomide/dexamethasone. His doctors have used up the major drugs that we like to use. Again, if you can get a patient like this on something new, like an ADC [antibodydrug conjugate] or something like that, that would be great. But the reality of availability is so minuscule compared with the denominator of need. I don’t think I’d feel comfortable giving this person elotuzumab/Revlimid/dexamethasone. I don’t think I’d feel comfortable.
C. Ola Landgren, MD, PhD:I would agree with that. If this patient came to see me in clinic, I would have the exact same perspective. We see these patients, unfortunately, quite often in our clinics. Ajai, you mentioned options such as DCEP [dexamethasone/cyclophosphamide/etoposide/cisplatin], VD-PACE [bortezomib/dexamethasone/cisplatin/adriamycin/cyclophosphamide/etoposide], and VDT-PACE [bortezomib/dexamethasone/thalidomide/cisplatin/adriamycin/cyclophosphamide/etoposide]. In my experience, they are quite efficacious to debulk the disease. The problem is, what are you going to do next?
You can do DCEP or VDT-PACE or VD-PACE. Then you need to have a plan in place. Could a patient then go to the CAR T-cell therapy? If the ECOG score was better, and the patient signed and wanted to go on therapy, you could collect the cells and then do DCEP, for example, and then go on to T-cell therapy. That could be a bridge toward that. But if the patient is not eligible, if you gave DCEP and had a response, and then, a month later, the disease is back again, what are you going to do now? So those are complicating situations. Could an allotransplant be an example? Is this something you would consider, Ajai?
Ajai Chari, MD:I have not been as impressed with allotransplantation. I would probably rather do a CAR T-cell therapy first, also because allotransplants are now excluded from many CAR T-cell studies as well. We have to think about sequencing more than we used to. Nina mentioned the antibodydrug conjugate. There are several targeted therapiesBCMA-targeting agents—with either bispecific or drug conjugates. The problem is, now you have to make a decision. Is the patient CAR T-cell–eligible or not? If you start using these antibodies that are targeting BCMA, they’re currently being excluded from CAR T-cell therapy. I think I would probably prefer a clinical trial.
We saw that in previous data that were presented by Amrita Krishnan. The CTN study compared autotransplantautotransplant versus autotransplant–allotransplant. There was really no benefit in all-comers. Even in the high-risk subgroup, at least as defined back then, this was not beneficial. So if we’re going to do allotransplants, it really has to be something innovative or thoughtful. Part of the problem is that many of our patients are older. They have renal dysfunction. They’re more prone to infections compared with those with other hematologic malignancies that do better with allotransplant. So I think we have a lot of issues.
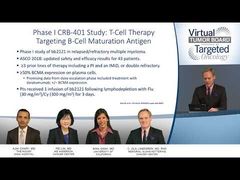
The one other point that is worth considering, and you kind of alluded to this in the data, is that if you think about every drug that’s been approved for myeloma, whether it’s bortezomib, carfilzomib, pomalidomide, lenalidomide, or daratumumab, they all work in about a third of patients for about 3 months in initial studies. Here we have a median of 7 prior lines of therapy giving a 95% response rate with a durability of almost 1 year. Admittedly, as you said, there were only 22 patients in this high cohort, but this is a really interesting signal. It’s a phase I trial. We are still learning more and are determining whether we should be using tocilizumab more empirically rather than waiting for people to get really sick. A lot of things still need to be worked out, but I think this is why there is so much interest in it. And clearly, this may move earlier if we see that the larger sample size substantiates that. I think that’s really important to consider.
One other thing that we didn’t talk about is that some patients are very cytopenic. Some patients can’t go into any clinical trial. Even DCEP could be challenging. As studied, these salvage transplants of remaining stem cells are a very effective way of resuscitating the hematopoiesis. In our study, about 70 patients had a median of 5 lines of prior therapy. They were extensively treated, and 75% of patients who are neutropenic or thrombocytopenic recovered counts such that they could then meet standard eligibility criteria. Again, we’re not going for durable responses. We’re just looking for trends in improvement.
C. Ola Landgren, MD, PhD:You cheer the patient up and kind of give a bridge into something else.
Ajai Chari, MD:Exactly.
C. Ola Landgren, MD, PhD:Nina, you brought up antibodydrug conjugates. Ajai talked about the fact that if you get even 1 dose of an antibody, that will cancel your opportunity to go on the trials for the BCMA CAR T cells. Let’s say the BCMA CAR T cells become approved in the near future. We hope for that. If a patient had received an antibody–drug conjugate and relapsed and had some other therapy, would you consider a BCMA-targeted CAR T-cell therapy, if it was an approved product?
Nina Shah, MD:There are no data on this, right? By definition, all these people have been excluded. But if you’re up against a wall and you really don’t know of anything else that has the chance of providing a remission, if it’s approved by standard of care and you can get coverage, I think that would be a reasonable alternative. To get them ready to collect enough lymphocytes and all these things, you may have to take them through a cycle of higher-dose chemotherapy, some stem cell rescue, etc. I agree with that. I don’t think it would be wrong to consider it. What do you think?
C. Ola Landgren, MD, PhD:I recognize that there are no data, so maybe it was...
Ajai Chari, MD:I think part of the answer to that question is scientifically driven, right? What is the mechanism of progression?
Nina Shah, MD:It may be different for the ADC versus CAR T-cell therapy.
Ajai Chari, MD:For CAR T-cell therapy, across the malignancies that have been studied so far, it’s not always antigenic loss. It could be productthe loss of the vector. So I think we really need to understand why patients progress on these targeted therapies to really answer that question.
Nina Shah, MD:From a reverse standpoint, it’s unfair, if people have gotten BCMA-directed CAR T-cell therapy, to be ineligible for ADC. Again, as you mentioned, it might not just be loss of BCMA. Maybe they’re rejecting the T cells or whatever else. So I really hope we can gain more intelligence about trial design to offer these therapies to more people.
C. Ola Landgren, MD, PhD:You think about the blocking of the 20S proteasome. We have both ixazomib and carfilzomib, and Velcade [bortezomib], going after the same subunits. So why couldn’t we use a target like BCMA? We need to know more. We need to learn more about these mechanisms and why the drug stops working, as you pointed out.
You pointed out that the patients treated here were on an average of 7 lines of therapy. They may not be cured with this therapy at this point. There needs to be more product development before we see better outcomes, but it’s still better than the 3 months we would expect to see, at best, with the other available options.
A subanalysis from this ASCO [American Society of Clinical Oncology] presentation showed that in patients who actually achieved MRD [minimal residual disease] negativity, the duration was 1.5 years. So it was even longer there. Maybe focusing on those mechanisms that really explain why the drug does or doesn’t work, and homing in on those patients to continue to develop CAR T cells could be a segue. And then, as you pointed out, Ajai, going even earlier. I’m sure we’d all agree that that’s where the field is headed.
Nina Shah, MD:Yes, not waiting until the last minute.
Ajai Chari, MD:From a patient’s perspective, it’s important to emphasize that this is a single intervention. There’s no ongoing therapy. From a treatment-free interval, quality-of-life point of view, for the patients who are in remission, they’re doing tremendously wellsome of whom would have gone to hospice.
C. Ola Landgren, MD, PhD:Right.
Nina Shah, MD:Absolutely.
C. Ola Landgren, MD, PhD:Thank you so much. This was a fun discussion.
Nina Shah, MD:Thank you.
Pei Lin, MD:Thank you.
Ajai Chari, MD:Thank you, Dr Landgren, Dr Lin, and Dr Shah, for your insight and thoughtful case presentations. To our viewing audience, thank you for joining us for thisTargeted Oncology Expert Perspective Virtual Tumor Board®presentation. We hope that you found this discussion to be informative and that you have acquired some practical knowledge that you can take back to your clinic. Thank you.
Transcript edited for clarity.
Advertisement
Related Content
Advertisement

































Advertisement
Advertisement
Trending on Targeted Oncology - Immunotherapy, Biomarkers, and Cancer Pathways
1
ASCO 2026 GU Cancer Highlights: Beyond the LBAs
2
Dr Tolaney on SG + Pembrolizumab Biomarker Data in First-Line mTNBC
3
FDA Approves Generic Eribulin Mesylate for Metastatic Breast Cancer
4
Bispecific ADC Iza-Bren Extends Survival in Advanced TNBC
5