
|Videos|January 28, 2020
Case 4: Treatment of Relapsed CLL
Advertisement
Episodes in this series

















EXPERT PERSPECTIVE VIRTUAL TUMOR BOARD
Anthony Mato, MD, MSCE:Well, this patient is progressing on ibrutinib, and now we are really going to delve into the question of sequencing. I’m curious, what would be the standard of care for a patient under these circumstances, assuming that there is no evidence of transformation?
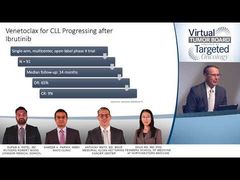
Sameer A. Parikh, MBBS:If we truly think that this is CLL [chronic lymphocytic leukemia] progression and that there is no evidence of transformation, the only prospective dataas we have talked about in 1 of the previous cases—are the data to suggest that venetoclax would be the treatment of choice in a situation like this. That was a single-arm phase II study, with venetoclax as the only agent used. Although the complete response rate was about 9%, the patients who got on that study had a median PFS [progression-free survival] of over 12 to 18 months.
Anthony Mato, MD, MSCE:I think it was about 24 months.
Sameer A. Parikh, MBBS:Twenty-four months, which I think is reasonable. I think this just tells us that if patients are progressing on ibrutinib, even the best treatment that we have now with venetoclax, you should be thinking about what is next. Particularly in our younger patients, because the expected benefit from venetoclax-based therapy is not going to be in the order of many, many years.
Anthony Mato, MD, MSCE:What about combinations, then? Venetoclax plus rituximab, for example. Experience there in that patient population? How do you decide then as a monotherapy or continuous, or do you give in combination?
Sameer A. Parikh, MBBS:That brings us to the discussion point for the MURANO study, which is the combination of venetoclax and rituximab compared with bendamustine and rituximab. This was a randomized phase III study that was done to compare the treatment options for these 2 groups of patients. This was in the relapsed setting, and it showed at the 4-year progression-free survival mark that the combination of venetoclax and rituximab did exceedingly well compared with bendamustine and rituximab.
It’s important to note that no patients who had had ibrutinib prior to getting on this trial were allowed. Patients who were progressing on ibrutinib-based therapy were not eligible to participate in this study. This is truly a patient population that has had progression on chemoimmunotherapy and went on the MURANO study. And the combination of venetoclax and rituximab was far superior to bendamustine and rituximab. After a median follow-up of 22 months, the 24-month progression-free survival was 75% in patients who receive venetoclax and rituximab. There was also a demonstrated overall survival benefit.
Anthony Mato, MD, MSCE:It’s interesting, though, that that patient population specifically really was completely BTK [Bruton tyrosine kinase] inhibitor naїve. We have to keep that in mind when trying to extrapolate those data to this particular patient with resistance of disease. Another topic that’s a little off our agenda for discussion would be other emerging agents to aid in this sequence. Thoughts on data from ASH [the American Society of Hematology 2019 Annual Meeting & Exposition]: We’re starting to delve into this area in which we have noncovalent BTK inhibitors that could potentially address this question. Should this patient have had aCys-481mutation, for example? Want to summarize what information we saw at the ASH meeting? I think that is not relevant to today, but it might be a few years into the future.
Sameer A. Parikh, MBBS:Those are very exciting data that were presented at ASH with the noncovalent BTK inhibitors. There are at least 3 that I’m aware of. There’s 1 by a company called [Loxo Oncology, Inc]. I think the agent is called LOXO.
Anthony Mato, MD, MSCE:305.
Sameer A. Parikh, MBBS:LOXO-305, thank you. The second one is an agent called ARQ 531, and a third one is vecabrutinib. All 3 agents have gone through their phase I dose-escalation study and have found that all these have reached potentially their maximum tolerated dose for the phase II portion of the study. A number of these agents have shown significant efficacy in patients who have had both theBTKC481Smutation as well as in the wild-type BTK protein, thereby suggesting that these would be potential treatment options for patients like this 1 who are progressing on ibrutinib-based therapy. Anthony, you had more data about the LOXO-305 study.
Anthony Mato, MD, MSCE:We presented that data at the ASH annual meeting, but it’s important, rather than focusing on the individual agents, to just highlight that there is an emerging class present. I’m also curious a little about Richter transformation because you mentioned this. I know your center has most recently presented data on identifying these patients. Do you want to comment a little on the data that you presented at iwCLL [international workshop on CLL] on how we identify a patient with Richter who’s progressing on a novel agent versus CLL?
Sameer A. Parikh, MBBS:I think that’s an important question, because in the pastin the chemoimmunotherapy era—when we thought about Richter transformation, we would typically do a PET [positron emission tomography] scan to try to understand what the maximum SUV uptake was. Generally speaking, it was thought that if the maximum SUV [standardized uptake value] was less than 10, then it was less likely that the patient had experienced a Richter transformation. If the SUV uptake was greater than 10, it was thought that that lymph node should be biopsied to make sure it was truly a Richter transformation and not really an infection or a second malignancy.
In the context of BTK inhibitors, we’ve noticed that there has been a change where a number of patients with a maximum SUV uptake of between 5 and 10and not necessarily only over 10—have also biopsy-proved Richter transformation. That calls into question this threshold that we’ve used in the past, where we would say our threshold of 10 would be to consider a biopsy or not. I think we’ve now slightly devised our approach, so if we have a patient who we think is progressing on a BTK inhibitorbased therapy and we do a PET scan, even patients who have an SUV uptake of 7 or 8 on a lymph node, we are more inclined to biopsy these patients to ensure that there is no Richter transformation.
Anthony Mato, MD, MSCE:That’s a really important point. In the relapsed/refractory setting with an early progressor like this, we really need to make that distinction. I think these have been 4 really interesting cases that have been presented. I want to thank Dr Ma, Dr Parikh, and Dr Patel for your thoughtful presentations and a lively informative discussion.
To our viewing audience, thank you for joining us for thisTargeted Oncology™Virtual Tumor Board®,presentation. We hope today’s discussion was a valuable use of your time and that you acquired some practical knowledge that you can take back to your clinic.
Transcript edited for clarity.
Advertisement
Related Content






























Advertisement
Advertisement
Trending on Targeted Oncology - Immunotherapy, Biomarkers, and Cancer Pathways
1
Updated HARMONi Analysis Shows Consistent OS Benefit With Ivonescimab in EGFRm Lung Cancer
2
FDA Accepts NDA for Daraxonrasib in Metastatic Pancreatic Cancer
3
How Inherited BRCA Mutations Shape Breast Cancer's Genomic Behavior and Point Toward a New Treatment Paradigm
4
First Patient Is Dosed in Trial of HLX-4310 for Relapsed/Refractory Osteosarcoma
5