Biomarker Testing Paves the Way for Better Targeted Therapies in NSCLC
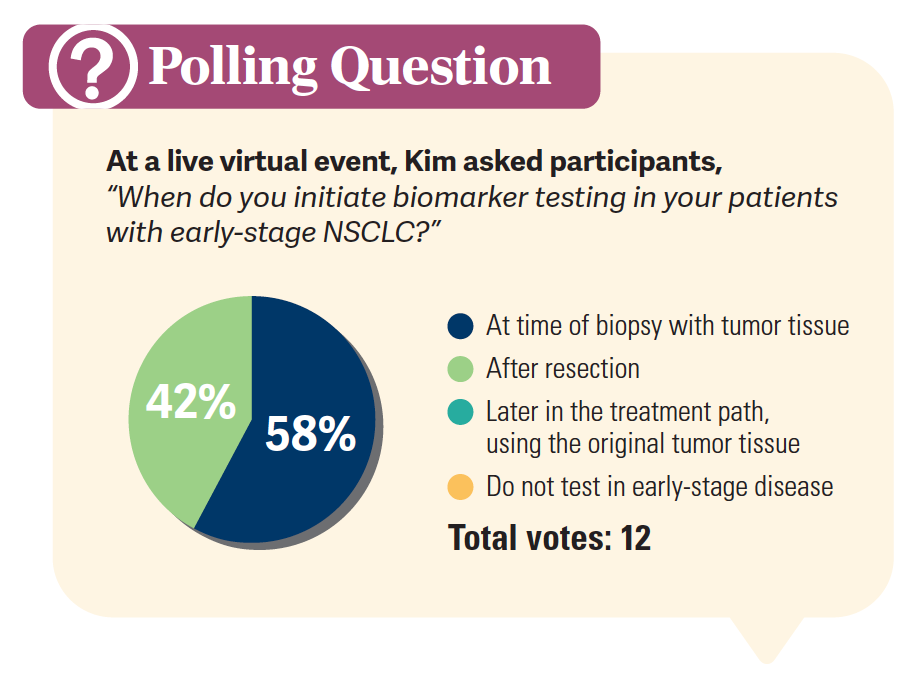
At a live virtual event, Edward S. Kim, MD, MBA, discussed the evolving landscape of biomarker testing before making treatment decisions for patients with early-stage non–small cell lung cancer (NSCLC).


Edward Kim, MD
Physician in Chief,
City of Hope Orange County
Vice Physician in Chief,
City of Hope National Medical Center
Duarte, CA

At a live virtual event, Edward S. Kim, MD, MBA, discussed the evolving landscape of biomarker testing before making treatment decisions for patients with early-stage non–small cell lung cancer (NSCLC).Biomarker testing has led to a change in treatment in this patient population, allowing targeted approaches to be used earlier and more aggressively. Kim also discussed the data behind some of these targeted therapies and how they’re impacting patients.
Importance of Biomarker Testing in NSCLC
We’ve observed that [the use of biomarker testing] is not as robust as we thought. Now, we’ve seen over time that the proportion of patients undergoing biomarker testing has risen, and risen more dramatically. In 2011 it was [approximately] 55%, and then in 2021 it was 88%.1 Although it’s getting better, this has become a situation, just like in [treatment for patients with] breast cancer, where for anyone who has a [cancer] diagnosis, we can’t treat them until we have the [biomarker tests] done. It’s the same thing in lung cancer now, where it’s becoming that we absolutely need these biomarkers to dictate which treatment direction we go in.
[When conducting biomarker testing for patients with] nonsquamous NSCLC, biopsy tissue or a cytology is adequate for molecular testing. If the tumor is resected, then you can [ follow the testing algorithm] and see what to do next.2 We’d love to have [the molecular panel] reflexively ordered by the pathologist—that’s why it works so well in breast cancer— but we know some of these panels require send-outs [and more involved steps]. If the tumor was not resected, then we would need to figure out another route around that and get a rebiopsy, if needed.2 We absolutely must have this testing and [the patient’s] histologic diagnosis, and then the molecular testing, at a minimum, needs to look for an EGFR mutation. We’d also like to see testing for ALK, but these tests are all on a panel these days. So it’s not that much more challenging to get [tests for] the…usual suspects and then get the immunohistochemistry reading. Still, there can be issues with local reimbursement, but these days, it’s very good to get the [molecular testing] panel [that’s available]. It doesn’t have to be the largest panel, but we know that there are certain important biomarkers that exist in lung cancer, and we know there are trials assessing these markers in certain settings.


Deciding on the Treatment Sequence
All patients should be evaluated for preoperative therapy, with strong consideration for nivolumab [Opdivo] or pembrolizumab [Keytruda] plus chemotherapy for these patients with tumors greater than or equal to 4 cm.3 And again, we need to test for their PD-L1 status and EGFR mutations and rearrangements [ for patients with] stage I through IIIB disease…. [When looking at neoadjuvant and adjuvant treatments], I don’t think…we have right vs wrong options here. That’s why the guidelines continue to expand, and there are a lot of different aspects to look at. When I was at [The University of Texas MD Anderson Cancer Center], we had a chair of surgery who was very much into induction…but that was in the early and mid-2000s [and things have certainly evolved]. It depends on who your surgical colleagues are that you’re working with and what they prefer.
And the data right now don’t tell you that one [approach] is better than the other, so I think it comes down to having a discussion. But whether it’s adjuvant chemotherapy, osimertinib [Tagrisso], atezolizumab [Tecentriq], or pembrolizumab…you’re just a little more gratified that [these options] even exist. Up until a few years ago, we really weren’t talking a lot about the [patients with] early-stage disease as far as having a medical intervention other than chemotherapy.
In biomarker-driven neoadjuvant treatment, you want to do your staging, look at surgical end points, and determine the tumor biopsy [because, again], the histology is very important. You [could then] consider neoadjuvant treatment there with chemotherapy plus an immune checkpoint inhibitor.4 You want to also run the biomarker tests, and if there are no driver oncogenes, then you can do the PD-L1 assessment, and [depending on those results], then you could consider neoadjuvant targeted therapy. Again, this is the paradigm for where we’re going with [treatment for these patients]. As we look at real-world adjuvant patterns,…as the stage [of the disease] increases, we’re doing more comprehensive treatment strategies to try to help the patients. This is the direction that we’re seeing that treatment is going.5
Practical Considerations
The first thing that I always look out for if I’m going to treat somebody who is outside of indication, [meaning] is not on the guidelines,6 is to make sure [the treatment is] reimbursed. You’d hate for someone to get an immunotherapy or tyrosine kinase inhibitor [TKI] and have to [take] it for a year, and then all of a sudden insurance isn’t going to pay for it. That’s my first concern with that aspect of it. It was less of a blow when it was just chemotherapy [ for these patients]. Ultimately, I think it’s going to be more of [treating someone outside the indications]…as we push the boundaries. [For example], if you have a patient who is 40 years old who has a 3.5-cm tumor and is EGFR positive, maybe you don’t want to give them chemotherapy and want to give them a TKI instead. So we’re going to continue to push those boundaries, because the drugs that we are [giving] are safer, easier to take, and don’t have the same type of [toxicities] as chemotherapy.7 [Right now], there’s no good answer around [treating outside the indications when we think it’s necessary], but [even if it’s done in some cases], I can’t espouse things that are not necessarily data-proven yet.
Efficacy of Osimertinib in NSCLC
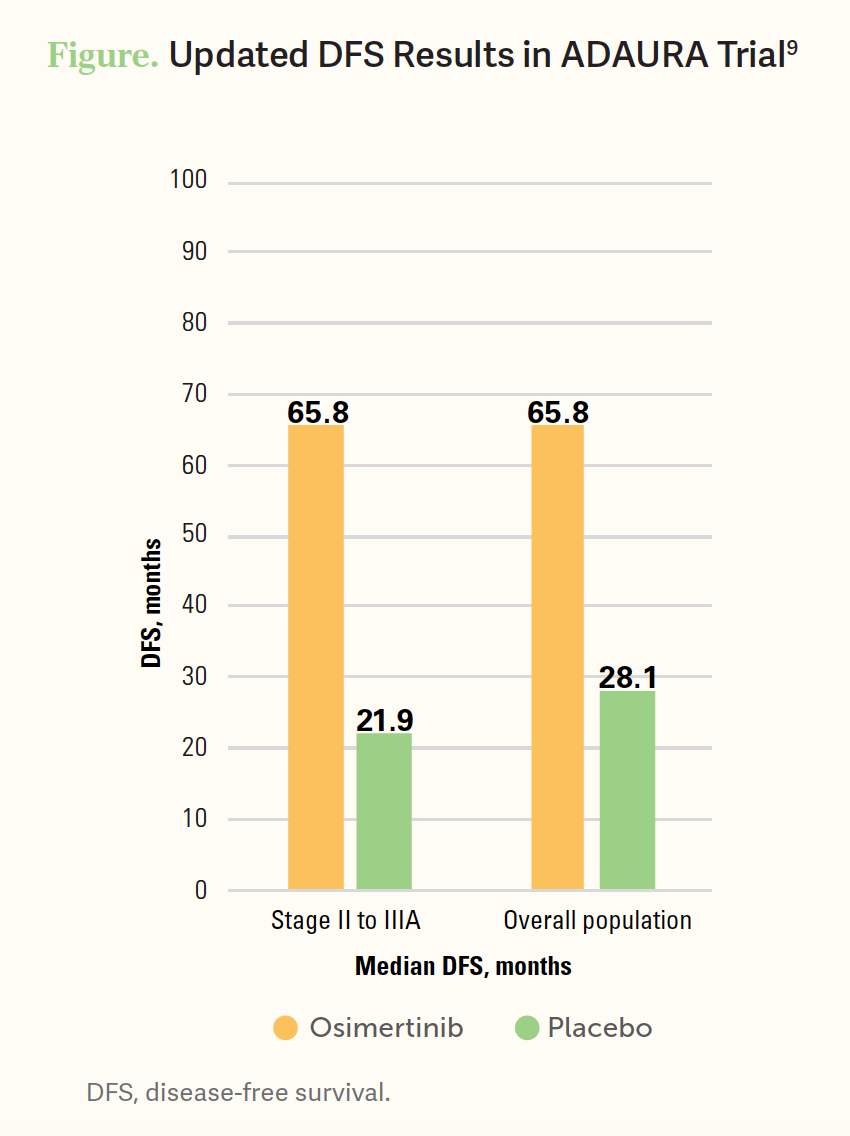
Even when these data [from the ADAURA trial (NCT02511106)] were about half mature [at the time of analysis], there were clear advantages [with osimertinib compared with placebo].8 Per stage of the disease, [the updated disease-free survival (DFS) results continued to be good (Figure9)]. In comparison, when we looked at this kind of stuff with adjuvant chemotherapy, we’d see minimal benefit in patients with stage IB disease. [The final overall survival (OS) analysis] was impressive [in osimertinib compared with placebo] with a 5-year OS rate of 85% [95% CI, 79%-89%] vs 73% [95% CI, 66%-78%], with an HR of 0.49 [95% CI, 0.33-0.73; P = .0004].9 We know that osimertinib has one of those special characteristics where even [with] an intact blood-brain barrier, it can cross into the central nervous system [CNS]. So when you look at the CNS incidences of relapse...there was obviously much more with placebo [with 29 of 41 patients experiencing a CNS event] and much less with osimertinib [with just 3 patients having a CNS event].9 When you look at all the OS subgroups [in this trial], it is pretty impressive, [such as a 0.49 HR (95% CI, 0.31-0.76) for patients with NSCLC with no smoking history].9 With the DFS HRs, just a couple of them crossed 1.0, if there was just a small sample size, but again, HRs from top to bottom were all very decent.9 When the patient’s relapse occurred, so not survival but looking at when their next event occurred, there was a big benefit of being on osimertinib.10


Safety Considerations With NSCLC
We have practiced with this drug in the metastatic setting for quite some time. It was one of the few instances where a higher-generation drug came with [fewer] adverse events [AEs]. So we’re used to sort of generations [of drugs] that went higher and higher [with AEs], and we saw a little more toxicity but with a corresponding improvement in efficacy. This was one of those drugs that was safe and easier to give, and we didn’t see much difference in the adjuvant setting as well, so it was very predictable. When focusing on grade 3/4 AEs, [there were just a few] of them. [There have been important] questions talked about interstitial lung disease, most notably with immunotherapy, but here we’re reporting it as 3% with osimertinib, and that was a concern early on when it came out.9
If you go to the original approval of osimertinib, there was a section that added some precaution against heart failure, which was very rare, but it was added into the indication where you wanted to test [the patient] to make sure that someone’s heart function was OK.11 As far as exacerbating a normal heart function, that would be a little unusual [to see with this therapy], but if somebody had some compromised heart function [as they start therapy], that’s where you want to be a little more cautious. [Clinicians] don’t really do it in practice, but that was on the original indication for osimertinib, [that if the patient] had some susceptibility to [heart issues, then you should] proceed with caution….10 I think it’d be unusual if someone who had a healthy normal ejection fraction [prior to treatment] then went into congestive heart failure…but exacerbating [the condition of] someone who already was compromised, that can happen [when giving osimertinib].
REFERENCES:
1. Yan JT, Jin Y, Lo E, et al. Real-world biomarker test utilization and subsequent treatment in patients with early-stage non-small cell lung cancer in the United States, 2011-2021. Oncol Ther. 2023;11(3):343-360. doi:10.1007/s40487-023-00234-7
2. Aggarwal C, Bubendorf L, Cooper WA, et al. Molecular testing in stage I-III non-small cell lung cancer: approaches and challenges. Lung Cancer. 2021;162:42-53. doi:10.1016/j.lungcan.2021.09.003
3. Martins RS, Razi SS, Alnajar A, et al. Neoadjuvant vs adjuvant chemoimmunotherapy for stage II-IIIB non-small cell lung cancer. Ann Thorac Surg. Published January 28, 2024. doi:10.1016/j.athoracsur.2024.01.004
4. Godoy LA, Chen J, Ma W, et al. Emerging precision neoadjuvant systemic therapy for patients with resectable non-small cell lung cancer: current status and perspectives. Biomark Res. 2023;11(1):7. doi:10.1186/s40364-022-00444-7
5. Friedlaender A, Addeo A, Russo A, Gregorc V, Cortinovis D, Rolfo CD. Targeted therapiesin early stage NSCLC: hype or hope? Int J MolSci. 2020;21(17):6329. doi:10.3390/ijms21176329
6. NCCN. Clinical Practice Guidelines in Oncology. Non-small cell lung cancer, version 2.2024. Accessed March 6, 2024. https://tinyurl.com/2x5sukut
7. Obradovic J, Todosijevic J, Jurisic V. Side effects of tyrosine kinase inhibitors therapy in patients with non-small cell lung cancer and associations with EGFR polymorphisms: a systematic review and meta-analysis. Oncol Lett. 2022;25(2):62. doi:10.3892/ol.2022.13649
8. Wu YL, Tsuboi M, He J, et al; ADAURA Investigators. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med. 2020;383(18):1711-1723. doi:10.1056/NEJMoa2027071
9. Herbst RS, Wu YL, John T, et al. Adjuvant osimertinib for resected EGFR-mutated stage IB-IIIA non-small-cell lung cancer: updated results from the phase iii randomized ADAURA trial. J Clin Oncol. 2023;41(10):1830-1840. doi:10.1200/JCO.22.02186
10. Tsuboi M, Herbst RS, John T, et al; ADAURA Investigators. Overall survival with osimertinib in resected EGFR-mutated NSCLC. N Engl J Med. 2023;389(2):137-147. doi:10.1056/NEJMoa2304594
11. FDA approves osimertinib for first-line treatment of metastatic NSCLC with most common EGFR mutations. FDA. Updated April 19, 2018. Accessed March 6, 2024. https://tinyurl.com/26n6p27y

















Roundtable Roundup: Treatment for Metastatic pMMR Endometrial Cancer
July 23rd 2024In separate, live virtual events, Michael J. Birrer, MD, PhD, and Jubilee Brown, MD, surveyed participants on the treatment of a postmenopausal woman with stage IVA endometrial cancer after first-line chemotherapy.
Read More


Depth of Response With Quadruplet Regimens Considered in Newly Diagnosed Multiple Myeloma
July 18th 2024During a Case-Based Roundtable® event, Timothy Schmidt, MD, and participants discussed treatment selection for a 54-year-old patient with transplant eligible R-ISS stage 2/R2-ISS stage 3 IgG-κ myeloma.
Read More
Rossetti Reviews Myelofibrosis Risk Stratification and Outcome Data for Pacritinib
July 17th 2024During a Case-Based Roundtable® event, James M. Rossetti, DO, discussed the role of risk scoring and stratification tools and treatment for a patient with declining hemoglobin and platelet counts due to primary myelofibrosis.
Read More

