Johnson Analyzes Combination Immunotherapy in the First Line in Advanced Melanoma
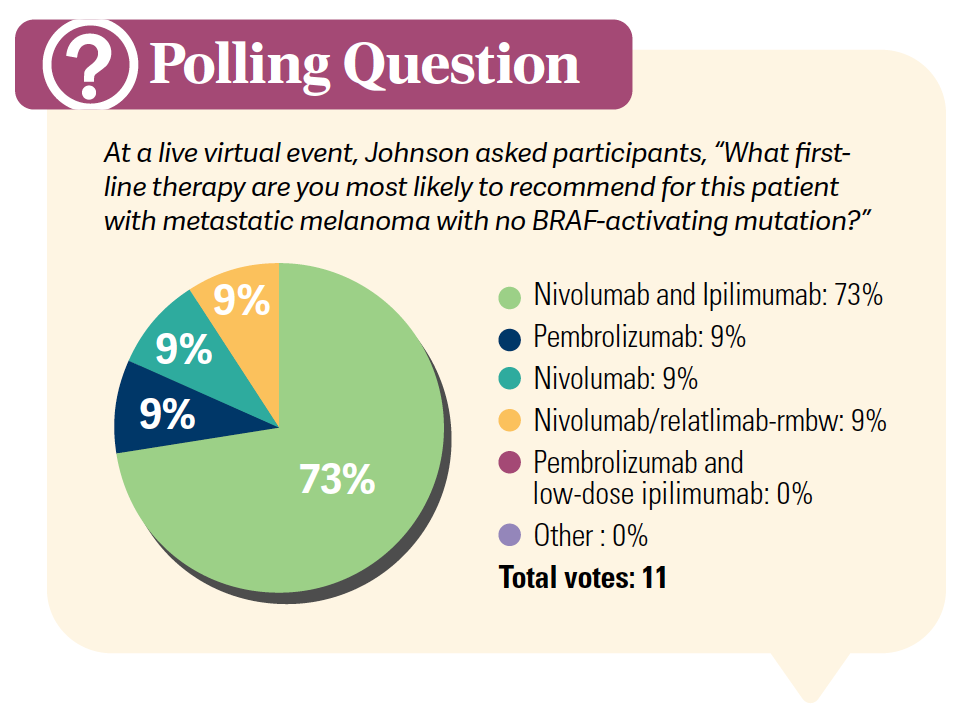
During a Targeted Oncology™ Case-Based Roundtable™ event, Douglas B. Johnson, MD, MSCI, reviewed data for safety and efficacy of immune checkpoint inhibition in patients with metastatic melanoma.


Douglas B. Johnson, MD, MSCI
Assistant Professor of Medicine of Hematology/Oncology
Vanderbilt University Medical Center
Nashville, TN

CASE SUMMARY
- A 78-year-old man with a history of stage III melanoma Underwent surgical resection 12 years prior
- Lymph node dissection (LND) positive for nodal involvement
- Patient declined complete LND and adjuvant systemic therapy.
- He has remained active since his surgery and maintains regular follow-ups.
- On routine follow-up, the patient now presents with moderate asthenia that is limiting his daily activities, without other relevant clinical symptoms.
- ECOG performance status: 1
- Physical examination was unremarkable.
- Notable laboratory findings: lactate dehydrogenase, 380 UI/L
- Full-body CT scan revealed the presence of pulmonary and hepatic nodules, with no evidence of brain metastases.
- He underwent core-needle biopsy of the largest hepatic lesion in segment IVb without any complications. Pathology revealed metastatic melanoma.
What are some key data that have come from the landmark clinical trials for treating patients with advanced melanoma?
JOHNSON: [Some of the key data to highlight] include the CheckMate 067 [NCT01844505] and the RELATIVITY-047 [NCT03470922] data. I think the first thing to highlight is the [high] overall response rate [ORR] with the combination of ipilimumab [Yervoy] plus nivolumab [Opdivo], [at 58%].1,2 Superficially, [with] nivolumab plus relatlimab-rmbw [Opdualag] the ORR seems to be more in line with a single-agent PD-1 [inhibitor], at 43%.3
However, there’s some nuance to that [finding]. The median progression-free survival [PFS] for nivolumab and relatlimab was, if anything, a little bit closer to that with ipilimumab and nivolumab in the CheckMate 067 data [at 10.22 months for nivolumab and relatlimab3 compared with 11.5 months for ipilimumab and nivolumab].1,2 What I think is also worth highlighting is the HRs, but there is always the danger of comparing across trials, because it’s not the same group of patients [in each one].
With CheckMate 067, the HR for PFS for ipilimumab plus nivolumab vs nivolumab alone was 0.79.1,2 Interestingly, with nivolumab and relatlimab, the HR was 0.78.3 So there was a similar benefit for the combination of nivolumab and relatlimab vs nivolumab, as was seen with ipilimumab plus nivolumab vs nivolumab alone. With ipilimumab plus nivolumab, as well as with monotherapy, there were impressive overall survival [OS] rates. Certainly, they exceeded 50% for ipilimumab plus nivolumab [at a median of 72.1 months; 52% at 5 years].1,2 In fact, even the 7.5-year survival rate was [48%],1,2 so there were impressive results across the [board] with PD-1–based therapies. The 2 combinations certainly seemed to improve that further.


Were there any central nervous system–specific data that came from these studies?
The answer right now is no, or, certainly, nothing systematic. There is an ongoing study of nivolumab and relatlimab for untreated brain metastases [NCT05704647], so hopefully within the next year we’ll have [expanded on] those data.4 I think for [patients with] brain metastases, and certainly untreated brain metastases, I would still not consider nivolumab and relatlimab equivalent to something like ipilimumab plus nivolumab, which has been studied much more in the context of brain metastasis.
The ORR with single-agent PD-1–targeted agents in untreated, nonradiated brain metastases, at least in small studies, is only approximately 20%. So single-agent PD-1–targeted agents don’t have a lot of activity. Now, I have many patients who were treated with stereotactic radiation or surgery and then got single-agent PD-1–targeted agents and did well. If a patient has had treated brain metastases, it’s a different situation.
Those patients can do well, but the primary response in untreated brain metastases seems to be quite rare. Now, just to round out the discussion, for the patients who are symptomatic or on steroids, ipilimumab gets a very low ORR: 5% in one study,5 but ipilimumab plus nivolumab certainly does not have great activity, [as well,] in patients with untreated brain metastases who are symptomatic or require steroids. For those patients, certainly you would want to do surgery or radiation, if possible, so that you could get them to a point where they could get off steroids or at least to a very low dose [of them].
What were the key safety outcomes from these landmark clinical trials in advanced melanoma?
I think it’s useful to compare across trials [and consider] the rate of severe toxicities with these different regimens. We certainly have the gestalt that shows the most severe toxicities are with ipilimumab plus nivolumab. This came from the results of the CheckMate 067 study, where you’re talking about the 3-mg/kg dose of ipilimumab.
Toxicities of grade 3 and grade 4 affected approximately 55% of patients.2 Almost all patients got some sort of immune-related or treatment-related toxicity, and approximately one-third of the patients discontinued treatment due to adverse events. If you compare that with the single-agent PD-1 inhibitor, 10% to 15% [of patients] will get a grade 3 or 4 toxicity, and just under 10% will discontinue due to toxicity.1,2
With nivolumab and relatlimab, the grade 3 and grade 4 toxicities [21%] were not much higher than with the single-agent PD-1 inhibitor. But approximately twice as many patients did discontinue therapy for toxicity [15%].3 You can think of nivolumab and relatlimab as being a lot less toxic than ipilimumab plus nivolumab but probably a bit more toxic than the single agent.
However, I think most people’s day-to-day experience with nivolumab and relatlimab is that it’s roughly similar to a single-agent PD-1 inhibitor. You don’t see nearly as much hypophysitis or colitis with this regimen, but you do see heightened PD-1 toxicities, whether it’s rash or hepatitis.3 Maybe hepatitis is not increased quite as much, but joint issues certainly can be elevated.
What were the overall results of the phase 3 RELATIVITY-047 trial?
This is the newest [study], which looked at patients randomly assigned to nivolumab vs fixed-dose nivolumab and relatlimab given as 1 infusion every 4 weeks.3 The primary end point was PFS by central review, not investigator review as in most of the other studies.
This was basically central review of the scans. The stratification factors included PD-L1 expression, BRAF mutation status, [and] disease stage. This was a well-balanced study in terms of age, gender, stage, performance status, and so forth.3
The overall results for both the study arm and the nivolumab arm3 weren’t quite as impressive as the results of the CheckMate 067 study.1,2 Maybe [this study had] a slightly sicker group of patients, but there was still an impressive Δ [at a median PFS of 10.22 months vs 4.63 months for the experimental and control arms, respectively]. The HR was 0.78, which is very similar to the HR for ipilimumab plus nivolumab vs nivolumab [0.79].1-3
Looking at the data by subgroup is always important, although you always have to take the results with a grain of salt because you could certainly slice and dice the data in a number of different ways. The results suggested, at least, that this regimen seemed to result in PFS improvement regardless of BRAF mutational status.3
In subgroups defined by LAG3 status, which was maybe not the best biomarker, there didn’t seem to be a huge difference. Yet, and this is worth exploring further, the regimen seemed to be beneficial in the group with low PD-L1 expression. Often with PD-L1, and in this study as well, I believe, you have divergent end points where you see some suggestion of PFS equivalence in the high–PD-L1 group, but you still have a higher ORR with the combination.
It’s a little hard to know how much to weigh those data.3 There was benefit in the groups with high and normal lactate dehydrogenase levels. There was benefit regardless of performance status, tumor burden, and baseline metastatic stage. There was also a low number of patients [with M0 disease], but there were similar HRs and similar point estimates for multiple different groups.3
[The researchers did] take a preliminary look at OS. These are still relatively immature data, but there were pretty similar results, at least as far as HRs and absolute Δ’s [median OS, not reached vs 34.10 months for the experimental and control arms, respectively; HR, 0.80; 95% CI, 0.64-1.01]. The HR does not meet significance at this point [P = .0593].
The CI almost breaks 1 but doesn’t quite do so. I think [the experimental regimen] certainly looks to be better, but I cannot say that with a lot of confidence, obviously, given that the study was not powered for OS.
We are at least now getting some hints that this regimen may be roughly as active as ipilimumab plus nivolumab. We certainly don’t have the long-term data yet, but we certainly have some hints.3
What did the results of this trial reveal about the efficacy of nivolumab and relatlimab with respect to ORR?
As I alluded, these were central review responses rather than investigator associated. The ORR was [43.1% vs 32.6% for the experimental and control arms, respectively].3 In CheckMate 067, the ORR was 58% vs 45%, respectively,1,2 so we see a roughly comparable difference in ORR. It may be a little higher with ipilimumab plus nivolumab, but it’s hard to say for sure. The rates of stable disease were [17.2% vs 16.4% in the experimental and control arms, respectively], and the rates of progressive disease were [29.6% vs 41.5%, respectively].3
What were the results of the safety analysis in RELATIVITY-047?
There was a bit more of pretty much every grade 3 and grade 4 adverse event [AE] and of overall AEs in the experimental arm than in the control arm but not dramatically more.
There was more grade 3 arthralgia and more grade 3 diarrhea, but the numbers were not tripled or quadrupled.3 I think it is [also] useful to break out the immune-mediated toxicities. It seems like there was not a lot of increased severe pneumonitis but maybe a tiny bit more hypophysitis [at 2 cases vs 1 case, respectively].
The rates of nephritis were equal; hepatitis and hyperthyroidism may be increased. Again, this is a slight increase of PD-1–associated toxicities, but it’s not dramatic. There were also 6 patients [1.7%] in the nivolumab and relatlimab arm with [myocarditis].3
REFERENCES
1. Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2019;381(16):1535-1546. doi:10.1056/NEJMoa1910836
2. Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. Long-term outcomes with nivolumab plus ipilimumab or nivolumab alone versus ipilimumab in patients with advanced melanoma. J Clin Oncol. 2022;40(2):127-137. doi:10.1200/JCO.21.02229
3. Tawbi HA, Schadendorf D, Lipson EJ, et al; RELATIVITY-047 Investigators. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. 2022;386(1):24-34. doi:10.1056/NEJMoa2109970
4. Phillips S, Burton EM, Kreidieh FY, et al. Phase II study of nivolumab (nivo) in combination with relatlimab (rela) in patients (pts) with active melanoma brain metastases (MBM). J Clin Oncol. 2023;41(16): TPS960. doi:10.1200/JCO.2023.41.16_suppl.TPS9605
5. Margolin K, Ernstoff MS, Hamid O, et al. Ipilimumab in patients with melanoma and brain metastases: an open-label, phase 2 trial. Lancet Oncol. 2012;13(5):459-465. doi:10.1016/S1470-2045(12)70090-6











Leon-Ferre Explores Targeting of PIK3CA Alterations in ER+ Breast Cancer
July 24th 2024During a live Community Case Forum event in partnership with the Minnesota Society of Clinical Oncology, Roberto A. Leon-Ferre, MD, discussed drugs targeting PIK3CA alterations in patients with ER+ metastatic breast cancer.
Read More


George Explores Impact of Risk Status With Cabozantinib/Nivolumab in Advanced RCC
July 19th 2024During a Case-Based Roundtable® event, Daniel George, MD, discussed the results of the CheckMate 9ER trial across favorable, intermediate, and poor risk groups in patients with advanced renal cell carcinoma.
Read More


Rossetti Reviews Myelofibrosis Risk Stratification and Outcome Data for Pacritinib
July 17th 2024During a Case-Based Roundtable® event, James M. Rossetti, DO, discussed the role of risk scoring and stratification tools and treatment for a patient with declining hemoglobin and platelet counts due to primary myelofibrosis.
Read More

Similar Efficacy in Melanoma Shown in Indirect Comparison of PD-1/LAG3 vs PD-1/CTLA-4
July 16th 2024During a Case-Based Roundtable® event, Michael A. Postow, MD, discussed an indirect treatment comparison of nivolumab plus relatlimab vs nivolumab plus ipilimumab in patients with advanced melanoma in the first article of a 2-part series.
Read More

