Lipson Considers Tolerability When Selecting Immunotherapy for Metastatic Melanoma
During a Targeted Oncology™ Case-Based Roundtable™ event, Evan J. Lipson, MD, and participants discussed tolerability factors that could influence the choice of frontline immunotherapy regimen for a patient with metastatic melanoma.


Evan J. Lipson, MD (MODERATOR)
Associate Professor of Oncology
Johns Hopkins Medicine
Baltimore, MD
PARTICIPANTS: Neeraj Mahajan, MD | Shyamal Bastola, MD | Tareq Al Baghdadi, MD | Elaine Beed, MD | Timothy Adamowicz, DO | Timothy Moore, MD | Michael Nemunaitis, MD | Samer Ballouz, MD | Baidehi Maiti, MD | Roopa Srikantiah-Saha, MD
EVENT REGION Michigan and Ohio
CASE SUMMARY
A 78-year-old man with a history of stage III melanoma underwent surgical resection 12 years ago; his lymph node dissection (LND) was positive for nodal involvement. The patient declined complete LND and adjuvant systemic therapy. He remained active since his surgery and maintained regular follow-up appointments.
On routine follow-up, the patient presented with moderate asthenia that limited his daily activities. His ECOG performance status was 1, and his physical examination was unremarkable. Notable laboratory findings included lactate dehydrogenase level of 380 U/L (reference range, 110-240 U/L). A full-body CT scan revealed pulmonary and hepatic nodules but no evidence of brain metastases. He underwent core needle biopsy of the largest hepatic lesion in segment IVb without any complications. Pathology revealed metastatic melanoma, and mutation testing showed BRAF wild-type disease.



LIPSON: In our clinic, we’d probably give this patient nivolumab/relatlimab [Opdualag]. We’re trying to avoid some of the serious toxicities you see with ipilimumab [Yervoy], especially full dose. And in a patient without brain metastases, we probably have a couple of shots on goal. If nivolumab/relatlimab didn’t do the trick and we needed to add ipilimumab to see whether that might help, we probably have time to do so.
MAHAJAN: I have used it in 1 patient. It is better than single-agent nivolumab [Opdivo] efficacy wise, but it has not been compared with ipilimumab/nivolumab. Tolerability wise, it is better than ipilimumab/ nivolumab but is still much more [toxic] than nivolumab alone. Ipilimumab/ nivolumab is difficult, but we also have a lot of experience with that now with the low dose of ipilimumab, especially in renal cell carcinoma and lung cancer. If you can get the patient through 4 cycles, then it becomes relatively easy [continuing] with single-agent nivolumab for those patients rather than using the combination [of nivolumab and relatlimab continually]. We have to also consider that angle.
BASTOLA: I have used it in 1 patient. If somebody can handle ipilimumab/nivolumab, that’s what I’m doing. All the patients for whom I was using [single-agent] nivolumab or pembrolizumab [Keytruda] are getting [nivolumab/relatlimab]. I still haven’t necessarily switched to use this drug in patients who I thought would get nivolumab/ipilimumab. And the longer we’re using it, the more patients I feel I can give…ipilimumab/nivolumab based on experience of handling it. I have a low threshold to drop the ipilimumab after 1 or 2 treatments if they have problems, because I feel like even if you get 1 or 2 ipilimumab doses, the patients will get long-term benefit. I don’t push all 4 doses if I can’t, but that’s how I would do it.
LIPSON: It does seem in some patients that you only need a little bit of ipilimumab. [After] 1 or 2 doses, you’ve activated an antitumor immunity, and sometimes that’s all you need. I remember a case back in 2015, I gave a single dose of ipilimumab/nivolumab. One time was all he needed, [although he had] some serious immune toxicity. It’s now 8 years later, and his liver tumor continues to shrink. He’s [been] off therapy…since 2015. Sometimes a little bit is all you need.
DISCUSSION QUESTIONS
- How do the rates of serious toxicities compare between different frontline immunotherapy regimens in patients with metastatic melanoma?
- What adverse events (AEs) stood out in the RELATIVITY-047 trial (NCT03470922) of nivolumab plus relatlimab?
LIPSON: The [grade 3 or 4] toxicity rate was 55% for full-dose ipilimumab/nivolumab in CheckMate 067 [NCT01844505].1 For nivolumab by itself [in the same trial], it was 16%. That’s probably slightly higher than some [trials], but pembrolizumab was around 10% [in KEYNOTE-006 (NCT01866319)] and nivolumab/relatlimab is in the middle, [at] 21% [Table1-3].


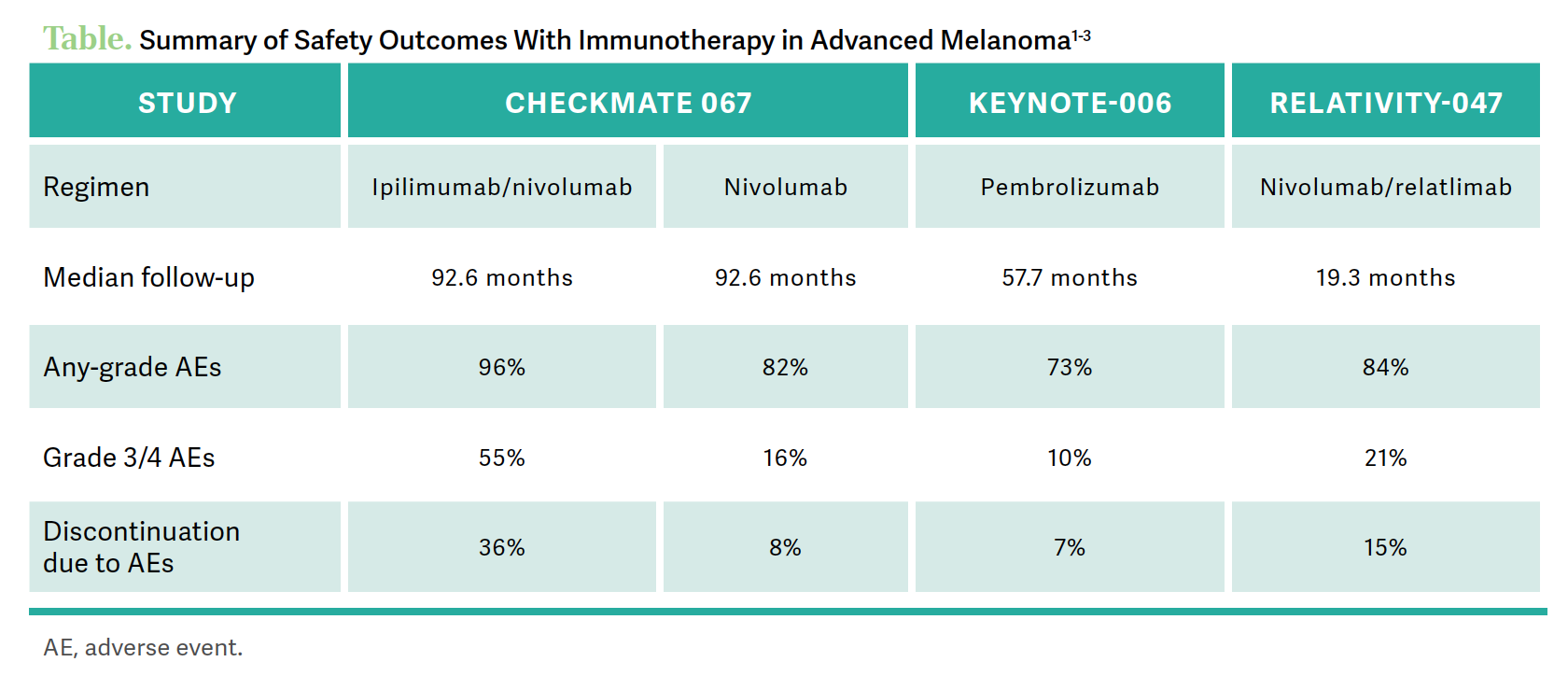
There was 1 additional AE of interest that didn’t shake out in the last year, and that is myocarditis. I’m not sure how many of you have seen myocarditis yet; it is fairly rare. Fortunately, there were only 6 patients of 350 or so who experienced that in the nivolumab/relatlimab arm. But when it does happen, it’s fatal in [approximately] half of cases, so myocarditis is [a concern].3 If somebody [presents] with shortness of breath, chest pain, new dyspnea on exertion, or anything that could be cardiac related, we are thinking about myocarditis, no matter which immune checkpoint inhibitor they’re getting—nivolumab/relatlimab, ipilimumab plus nivolumab, or pembrolizumab.
AL BAGHDADI: Do you do any specific monitoring? Because during the drug development of relatlimab in combination with nivolumab, they always saw some myocarditis. It seems to happen slightly more frequently with that combination. We were writing a trial in bladder cancer, and I thought about implementing cardiac monitoring. Do you do anything specific in that regard, or do you wait and let the clinical variables guide you?
LIPSON: In the trial, we tested troponins in everybody regardless of symptoms. For us, it was more confusing than helpful. A patient would come in and a troponin would be just slightly above the upper limit of normal, and you didn’t know whether the patient had just been particularly active the before and had a slight troponin leak or it was indicative of impending myocarditis. Based on that, we don’t test unless somebody comes in with symptoms. However, I’ll say that we have a low threshold. For anything that…could be myocarditis, we should [check] troponins, creatine [phosphokinase], and get an electrocardiogram.
DISCUSSION QUESTIONS
- How has your comfort level in managing immune-related AEs in the setting of metastatic melanoma changed over time?
- Do you refer to guidelines or protocols to manage immune-related AEs in metastatic melanoma?
- To what extent does ease or difficulty of managing potential toxicities factor into your recommendations?
BEED: I used pembrolizumab [nearly] the first day it came out. I’ve had really good luck until [I used] ipilimumab/ nivolumab. I’ve always had problems no matter what I did; it seemed like the patient [would have] a terrible reaction the first time and then end up not wanting to do it again. Unfortunately, after using [immunotherapy] all these years, I had my first cardiotoxicity. This was a working teacher [who was] fairly young—almost 60 [years old]—and… they transferred her to a larger hospital because she coded 3 times. She needed a pacemaker, rehab, and high-dose steroids.… In all those years, that was the only one, and she did make it, but it was touch-and-go. I was a little surprised [because] she was not the person you [would think would] have a cardiac problem.
LIPSON: It is very hard to predict it. It’s not the patients who have known coronary disease with an ejection fraction of 40% and had a myocardial infarction 2 years ago.
BEED: I’ve had patients older than 90 years, and they do really well on [immunotherapy]. You hate to put them on something too strong….
ADAMOWICZ: This is where we appreciate the specialists in their respective fields to teach us about how to use drugs like relatlimab. But in dealing with toxicity of immunotherapy in general, we’re getting very good at it. We use these types of drugs across the board in almost every disease state, and every disease state has its own nuances. The toxicities all have their own importance in different situations. But in the community, we’re getting really good at it. Early detection, a good review of systems, and a fair physical examination can get you way ahead of the game. I’ve seen some horrible toxicities from these drugs, but I don’t have any stories like they did in the first year or 2, when we used these before we knew what to look for.
LIPSON: I wonder whether anybody has come across the “terrible triad.”
ADAMOWICZ: I have seen it. The patient got out of that, but he ultimately died of his disease. He had myocarditis, which was fairly mild. He presented with pretty significant myasthenia gravis, but he also had some myositis, and his creatine phosphokinase was pretty elevated. I’ve seen 3 cases of myasthenia gravis now, so I’ve developed an understanding of how to get those patients managed.
LIPSON: The terrible triad is myositis, myasthenia gravis, and myocarditis. And for whatever reason, they run together sometimes. If you see one, it’s important that you look for the other two; they have a fatality rate close to 50%.
MOORE: We commonly use ipilimumab at a dose of 3 mg/kg in melanoma vs 1 mg/kg in renal cell carcinoma, for example. I’m always curious why we’re doing it that way, because 1 mg/kg of ipilimumab is much more tolerable than 3 mg/kg.
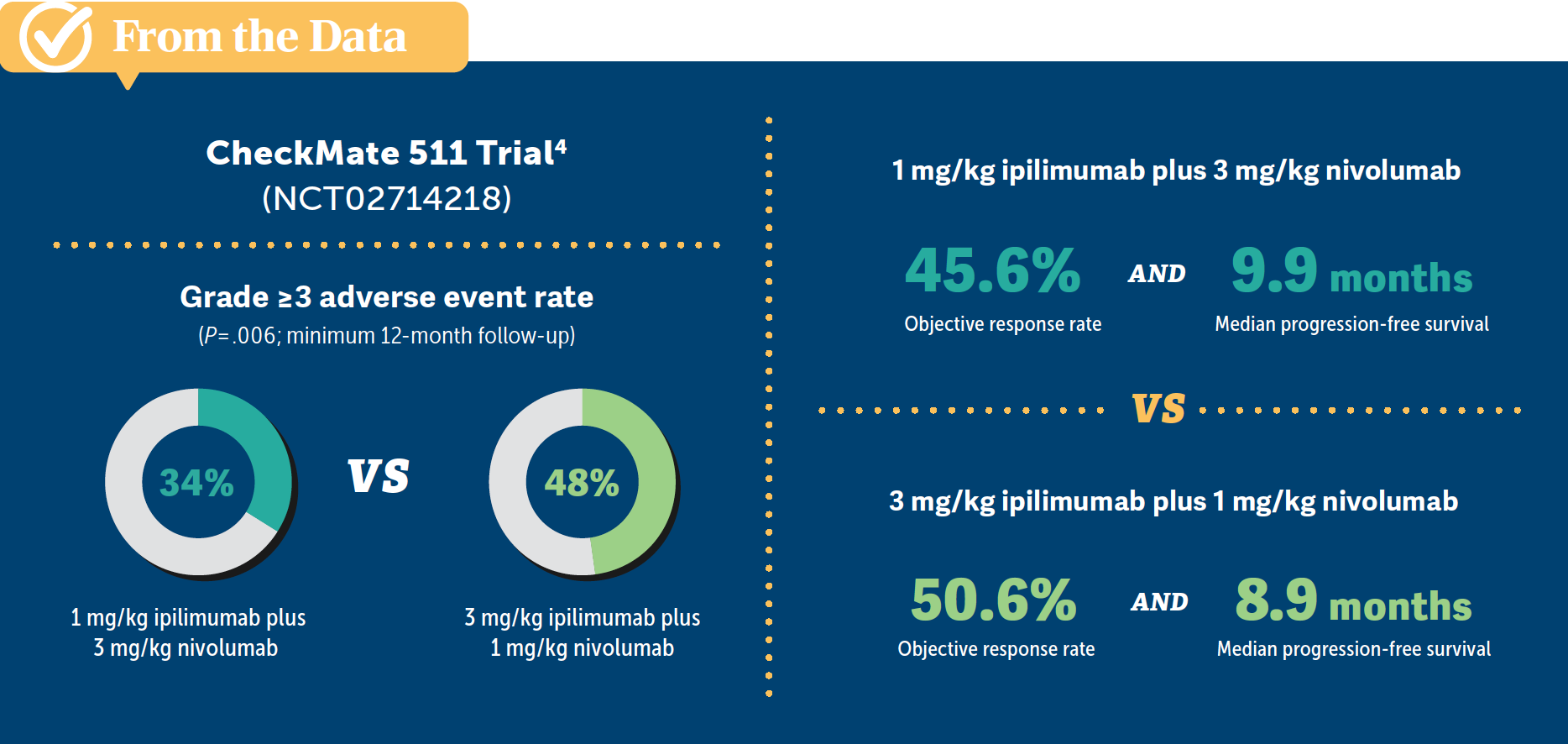
LIPSON: There was a study that compared low-dose ipilimumab [with] regular-dose ipilimumab and nivolumab, called the CheckMate 511 study [NCT02714218]. The good part is that it was powered to understand whether there was a difference in toxicity between the 2 regimens. The limitation of that study is that it was not powered to look at a comparison of efficacy between those 2. The toxicity difference is real. There’s a [48%] serious toxicity rate with full-dose 3 mg/kg of ipilimumab, which drops to [34%] when you look at 1 mg/kg of ipilimumab.4
Some other secondary end points on that study included overall survival, progression-free survival [PFS], and duration of response. [It] looks like they are in the same ballpark, but the trial was not powered to compare them [From the Data4]. In that study, they look approximately the same, but can we say for certain that there isn’t a dose-decreased response by dropping the dose? We don’t know for sure. We [also] have limited data using low-dose ipilimumab in patients with brain metastases. That is one situation where I almost never drop the dose. But I, too, am concerned about toxicity in some of the older patients with comorbidities and will occasionally drop the ipilimumab dose for the reasons we’re discussing.


DISCUSSION QUESTIONS
- How do you balance efficacy, safety, patient preferences, goals of therapy, and quality of life when recommending a first-line regimen?
- Do you confront any barriers to using a new immunotherapy option?
NEMUNAITIS: I haven’t seen too many melanoma cases in the past 6 months, but it seems like the relatlimab doesn’t add much more toxicity, and everybody’s had ipilimumab toxicities that we’re afraid of at times. Anytime I can [avoid using] ipilimumab, I’m happy, so it’s something I’ll use in practice when it comes up.
BALLOUZ: Like any other disease, you always balance the efficacy and toxicity. I learned my lesson in melanoma. I have good success with a combination of ipilimumab and nivolumab. I try to push for it if I think it is appropriate, and I have a lot of success stories with patients living years without any problems. My bias is to push for it. I’m very comfortable managing the toxicity. I have patients who ended up in the hospital with their treatment, but at the same time, the same patient…has no evidence of disease 3 years later.
ADAMOWICZ: Another thing that doesn’t get emphasized enough in these discussions is that the patients who do have the immune-related AEs can have better responses. Anytime I get a patient with a mild immune-related AE, I try to emphasize the silver lining that you have a 3-times better PFS if you try to basket these trials together. I don’t know whether that specifically holds true for melanoma, but I look at the lung cancer data, and they are quite impressive.5
LIPSON: It is true for melanoma.6 When [a patient presents] with a bad toxicity, we say, “We have to hold therapy, but don’t be too upset; this is a good sign.” The immune system is activated, it attacks cancer, [but] it attacks normal parts of the body. It’s all the same process.
MAITI: I personally have not had a chance to use relatlimab/nivolumab, but I’m not aware of any barriers. We have pretty good access for most patients. If I see an older patient with comorbidities, especially a history of autoimmune disorders that are well controlled, I’ll lean more toward nivolumab/relatlimab vs ipilimumab/nivolumab.
SRIKANTIAH-SAHA: We don’t have a specific protocol that we have to follow, but we do have some patients who come from a distance. A lot of [the challenge] is managing some of the AEs. And in some of those older patients where we tend to use just the PD-1 inhibitor, I would feel more inclined to add relatlimab vs ipilimumab.
REFERENCES
1. Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. Long-term outcomes with nivolumab plus ipilimumab or nivolumab alone versus ipilimumab in patients with advanced melanoma. J Clin Oncol. 2022;40(2):127-137. doi:10.1200/JCO.21.02229
2. Robert C, Schachter J, Long GV, et al. Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med. 2015;372(26):2521-2532. doi:10.1056/NEJMoa1503093
3. Tawbi HA, Schadendorf D, Lipson EJ, et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. 2022;386(1):24-34. doi:10.1056/NEJMoa2109970
4. Lebbé C, Meyer N, Mortier L, et al. Evaluation of two dosing regimens for nivolumab in combination with ipilimumab in patients with advanced melanoma: results from the phase IIIb/IV CheckMate 511 trial. J Clin Oncol. 2019;37(11):867-875. doi:10.1200/JCO.18.01998
5. Zhao Z, Wang X, Qu J, et al. Immune-related adverse events associated with outcomes in patients with NSCLC treated with anti-PD-1 inhibitors: a systematic review and meta-analysis. Front Oncol. 2021;11:708195. Published September 15, 2021. doi:10.3389/fonc.2021.708195
6. Serna-Higuita LM, Amaral T, Forschner A, et al. Association between immune-related adverse events and survival in 319 stage IV melanoma patients treated with PD-1-based immunotherapy: an approach based on clinical chemistry. Cancers (Basel). 2021;13(23):6141. doi:10.3390/cancers13236141












Leon-Ferre Explores Targeting of PIK3CA Alterations in ER+ Breast Cancer
July 24th 2024During a live Community Case Forum event in partnership with the Minnesota Society of Clinical Oncology, Roberto A. Leon-Ferre, MD, discussed drugs targeting PIK3CA alterations in patients with ER+ metastatic breast cancer.
Read More


George Explores Impact of Risk Status With Cabozantinib/Nivolumab in Advanced RCC
July 19th 2024During a Case-Based Roundtable® event, Daniel George, MD, discussed the results of the CheckMate 9ER trial across favorable, intermediate, and poor risk groups in patients with advanced renal cell carcinoma.
Read More


Rossetti Reviews Myelofibrosis Risk Stratification and Outcome Data for Pacritinib
July 17th 2024During a Case-Based Roundtable® event, James M. Rossetti, DO, discussed the role of risk scoring and stratification tools and treatment for a patient with declining hemoglobin and platelet counts due to primary myelofibrosis.
Read More

Similar Efficacy in Melanoma Shown in Indirect Comparison of PD-1/LAG3 vs PD-1/CTLA-4
July 16th 2024During a Case-Based Roundtable® event, Michael A. Postow, MD, discussed an indirect treatment comparison of nivolumab plus relatlimab vs nivolumab plus ipilimumab in patients with advanced melanoma in the first article of a 2-part series.
Read More

