
|Videos|January 28, 2020
Case 1: Assessing Risk in CLL
Advertisement
Episodes in this series

















EXPERT PERSPECTIVE VIRTUAL TUMOR BOARD
Anthony Mato, MD, MSCE:I guess you’ve all encountered the same situation before. Well I personally think you presented enough information for this patient that I think treatment is warranted. we’ve kind of touched on risk stratification. When you’re seeing a new patient, I’ll through this out to the group, how are you assessing risk? What is mandatory to be tested in order to decide how to move forward?
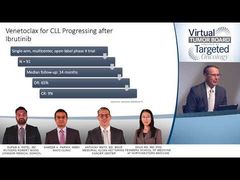
Shuo Ma, MD, PhD:The first thing is clinical staging. We all know that in the United States we use the Rai Staging System to locate patient who has only lymphadenopathy, sorry, lymphocytosis without anything else. That’s the low-risk group of patients. If they have lymphadenopathy, hepatosplenomegaly that will be the intermediate risk group of patients. Or for patients who are, such as this, who also has a cytopenia, anemia and thrombocytopenia due to bone marrow infiltration, that’s high-risk Rai stage patients. In Europe, Binet staging is being used in a very similar fashion.
The clinical staging has been established for many years and it still has the important guidance, one of the risk assessment criteria.
I know we kind of touched on the other risk assessments as well. I think fluorescence in situ hybridization [FISH], so peripheral blood FISH study is a very important FISH, uh, a prognostic, but also pretreatment is very important to realize that patients’ FISH panel can potentially change from the time of diagnosis. Even if your patient already had a FISH study done at diagnosis, it’s usually recommended to repeat that because they could acquire novel genetic changes that might change our treatment decisions.
Anthony Mato, MD, MSCE:Does anybody have an arbitrary cut-off for how long has to relapse before you need to repeat the test? Let’s say the patient was diagnosed 6 months ago and they’re treated now. Do you repeat? Do you not? I don’t know that I have an answer to this but since we’re here I’m curious what your thoughts are.
Sameer A. Parikh, MBBS:You’re right, there is not right answer. We’ve typically used a cut-off of between 2 to 3 years. But that’s completely arbitrary. I don’t have any data to suggest that things will not change in 6 months or they will change in more than 3 years. I think that’s the general cutoff that we’ve used.
Anthony Mato, MD, MSCE:For repeat testing.
Sameer A. Parikh, MBBS:Now that’s between diagnosis and first treatment. But between first and subsequent line therapy, we would always repeat a FISH panel for, for obvious reasons.
Anthony Mato, MD, MSCE:Totally agree. What about [next-generation sequencing (NGS)]sequencing, is that mandated?
Sameer A. Parikh, MBBS:We do not have a next generation sequencing test that we do on all our patients because the only one that we actually do would be aTP53mutation sequencing study because it has implications for a treatment choice perspective and …to counsel patients for how long any treatment response is likely to last. Other mutations may be prognostic but currently are not “actionable,” such asNOTCH 1,SF3B1, etc. We do not routinely get those for all our patients.
Anthony Mato, MD, MSCE:But everyone here getsTP53mutational status.
Shuo Ma, MD, PhD:Now we’re starting to, yes.
Anthony Mato, MD, MSCE:OK.
Shuo Ma, MD, PhD:Then as we already discussed with this patient,IGVHmutation status, that is also a very important factor when you’re considering treatment.
Transcript edited for clarity.
Advertisement
Related Content
















































Advertisement
Advertisement
Trending on Targeted Oncology - Immunotherapy, Biomarkers, and Cancer Pathways
1
FDA Clears Pen Device for Interferon Therapy in Polycythemia Vera
2
FDA Rejects Edotreotide PET Imaging Kit Over Manufacturing Concerns
3
Deep Responses Support Push for CAR T-Cell Therapy in AL Amyloidosis
4
FDA Accepts RP1 BLA Resubmission for Advanced Melanoma
5