
|Videos|January 28, 2020
Case 1: The Use of Ibrutinib in CLL
Advertisement
Episodes in this series

















EXPERT PERSPECTIVE VIRTUAL TUMOR BOARD
Anthony Mato, MD, MSCE:This patient was unmutated, correct?
Shuo Ma, MD, PhD:Yes, with an 11q deletion.
Anthony Mato, MD, MSCE:We’re going to talk about treatment choices, but chemoimmunotherapy for unmutated patients, is that something that’s considered still or are we going down the road of targeted therapies for this patient?
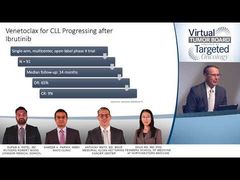
Shuo Ma, MD, PhD:I think based on the data from the last several years we can say confidently that forIGVHunmutated patients, the novel targeted therapies definitely outperform the conventional immunochemotherapy. This was demonstrated by several large randomized clinical trials. We can… look at some of the most important clinical trials. The Bruton tyrosine kinase [BTK] inhibitor, ibrutinib, … the first to be approved on the market, has been used for the past 4 or 5 years. There are quite a few large randomized clinical trials in the first-line setting. The first 1 that established the role of ibrutinib as single-agent is the RESONATE-2 study when the previously enrolled elderly chronic lymphocytic leukemia [CLL] patient was randomized between single-agent ibrutinib as a continuous treatment versus chlorambucil single-agent.
In that study, ibrutinib has shown significant improvement of progression-free survival over the conventional chlorambucil treatment. That was the first trial that established the efficacy of this treatment and it allowed ibrutinib to receive an FDA approval as a frontline treatment for CLL.
As well all know, in the United States chlorambucil single-agent is not really a very popular regimen, unless it’s a very elderly patient with lots of comorbidities. Then more commonly used immunochemotherapy combinations or fludarabine, cyclophosphamide, and rituximab [FCR] for therapy that cyclophosphamide in combination with rituximab, or the bendamustine in combination with rituximab. Sameer, would you like to touch on those studies and compare?
Sameer A. Parikh, MBBS:Sure, those 2 were major trials that were presented at the ASH Annual Meeting in 2018 and have subsequently been both published as full-length articles in theNew England Journal of Medicine[NEJM]. The first study was the E1912 study, which was the ECOG study that randomized younger patients, less than 70 years of age, to a 2 weeks-to 1 randomization to either receiving ibrutinib at standard doses on an indefinite basis, versus 6 cycles of fludarabine, cyclophosphamide, and rituximab.
Important to note that patients with deletion-17p were excluded from this particular trial. After a median follow-up of approximately 31/2 to 4 years ibrutinib showed a better, the combination of ibrutinib and rituximab actually in this trial showed a better progression-free survival. In fact, even a better overall survival compared to fludarabine, cyclophosphamide and rituximab. Thus this trial actually was in many ways an important practice changing trial, particularly for the young patients where FCR was being considered.
The one subgroup of patients where you would still have FCR as a discussion point would be in the young patients who have low-risk fluorescence in situ hybridization [FISH] profile, such as deletion 13q or perhaps trisomy 12, and have mutatedIGVHgenes because there wasn’t a significant difference in the progression-free survival and the overall survival between the groups of patients who received either ibrutinib or FCR.
Anthony Mato, MD, MSCE:We keep talking about young patients, do you want to sort of paint the context what’s young here in terms of fludarabine-based therapy?
Nupam A. Patel, MD:I will typically use 65 years of age as a cutoff for a young patient, although this particular trial allowed patients up to 70 years of age to be enrolled, but the median age I think was 58 in this study. It’s typically a patient who’s less than 65 years of age.
The companion trial was the Alliance [A041202] trial that randomized patients to 1 of 3 arms, either ibrutinib as a single agent; ibrutinib in combination with rituximab; or bendamustine and rituximab. The median age of enrollment of patients in this trial was about 72 years, and there was an improvement in progression-free survival and overall, excuse me, progression-free survival only in the ibrutinib-containing arms compared with bendamustine and rituximab, which again was important information because it showed that ibrutinib containing regimens outperformed standard chemotherapy that was used in our older patients with CLL.
Anthony Mato, MD, MSCE:Before we get to the sort of the twists and turns to use of ibrutinib when-whether it should be given in combination or a single, somebody want to just talk about how they get it, what’s the dosing, what’s the schedule? Is it given continuously? Is there any time-limited approach that’s approved or been studied yet?
Shuo Ma, MD, PhD:Yes, so ibrutinib, the standard FDA-approved dosage is 420 mg orally once a day, and it’s supposed to be used continuously until disease progression, or until intolerable toxicity. There has not really been time-limited study to demonstrate that’s feasible, although there were patients who had to come off treatment due to toxicity. This year at the ASH Annual Meeting in 2019, there was a small analysis showing that for patients who initially responded but later have to come off treatment, I think they were on treatment for a median of something like 18 months to close to 2 years. And then when they came off treatment they can actually, many of the patients can remain progression free for.
Anthony Mato, MD, MSCE:A couple of years.
Shuo Ma, MD, PhD:Two years to 3 years. Those are the patients who had the disease well controlled by the time they came off treatment. If they’re different, if you have a patient who had to come off treatment when their disease is still very active. Those patients from our clinical observations said those patients tend to progress quickly when they come off treatment. Unless if a patient has intolerable toxicity, we do not recommend to stop the ibrutinib treatment.
Transcript edited for clarity.
Advertisement
Related Content
















































Advertisement
Advertisement
Trending on Targeted Oncology - Immunotherapy, Biomarkers, and Cancer Pathways
1
FDA Clears Pen Device for Interferon Therapy in Polycythemia Vera
2
FDA Rejects Edotreotide PET Imaging Kit Over Manufacturing Concerns
3
Deep Responses Support Push for CAR T-Cell Therapy in AL Amyloidosis
4
FDA Accepts RP1 BLA Resubmission for Advanced Melanoma
5