
|Videos|September 25, 2018
Case 3: Aggressive Relapse of Multiple Myeloma
Advertisement
Episodes in this series













EXPERT PERSPECTIVE VIRTUAL TUMOR BOARDAjai Chari, MD:We’ve reviewed 2 cases so farfor newly diagnosed treatment and maintenance therapy post transplant. Here, we’re going to move to aggressive relapse of myeloma. We’ll start with a case of a 54-year-old African American woman. In May of 2014, she presented with fatigue and back pain. Her only past medical history was hypertension and mild renal impairment. Her hypertension was being managed on losartan. Her labs were significant for mild anemia. Results revealed a hemoglobin of 11.4 g/dL, with a calcium slightly on the upper limit of normal—11.1 mg/dL. Her albumin was normal—3.6 g/dL—and her creatinine was slightly elevated at 1.5 mg/dL. She had a monoclonal protein at 0.8 g/dL; an elevated beta-2 microglobulin, at 5.2 mg/L; and her LDH [lactate dehydrogenase] was 122. Her MRI [magnetic resonance imaging] did confirm multiple lytic lesions in her vertebrae, and her marrow confirmed the diagnosis of myeloma. She was found to have revised ISS [International Staging System] stage II disease with a t(11;14) translocation.
She was treated with RVd [lenalidomide (Revlimid)/bortezomib (Velcade)/dexamethasone] for 6 months and achieved a partial response. Following systemic therapy, she underwent an autologous stem cell transplant. After a discussion regarding the risks and benefits, the patient declined maintenance therapy. Now, about 2.5 years later, we find that she has relapsed with an M spike of 0.6 g/dL. Subsequently, in June of 2017, approximately 6 months later, her M spike was 1.7 g/dLso we saw relatively rapid doubling. She was started on daratumumab, lenalidomide, and dexamethasone, and she achieves a very good partial response.
Unfortunately, in July of 2018, her MRI shows new lytic lesions, although she has a good performance status. At this time, her labs show a hemoglobin of 11.5 g/dL, a calcium of 9.8 mg/dL, good renal function (1.1 mg/dL), and an M spike of 1.1 g/dL. Her beta-2 microglobulin is 5.6 mg/L. She did undergo a repeat bone marrow biopsy that identified del(17p)not detected initially—in 50% of cells, in addition to the previously identified t(11;14) translocation.
This patient with relapsed disease brings up questions on a very difficult area of myeloma management. How do you practice evidence-based therapy when there are so many regimens, all of which have been published in high-impact journals? To start, we really have to think about the backbone regimens for which these studies were done. We can broadly divide them into lenalidomide backbone-containing regimens versus proteasome inhibitorsPIs.
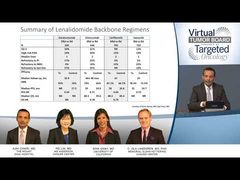
We have 4 excellent phase III studies, all published in high-impact journals, comparing Rd [lenalidomide/dexamethasone] with the addition of a novel therapy. We have the POLLUX study, where daratumumab was added; the ELOQUENT study, where elotuzumab was added; ASPIRE, where carfilzomib was added; and TOURMALINE, where ixazomib was added. All of these studies looked at large numbers of patients, ranging from 570 to 800 patients.
The next rows of the table really highlight what we are told in medical schoolwe should not compare studies directly to each other because the patient populations are different. Distilled here are some salient features of the rates of ISS stage III disease, which can be as low as 12% to 21%. High-risk FISH [fluorescence in situ hybridization] can be as low as 13% to 30% with 1 or 2 lines of therapy. Importantly, refractoriness to backbone regimens can be really important in these different regimens. With the PI-containing regimens—carfilzomib and ixazomib—we’re not going to have as much refractoriness to the PI, and some of those are probably protocol exceptions, whereas with daratumumab and elotuzumab, about 20% of patients were PI refractory.
When you look at IMiD [immunomodulatory imide drug] refractoriness, again, by definition, none of these patients could have been refractory to lenalidomide. Otherwise, they would not have been appropriate to randomize to receive lenalidomide/dexamethasone. And so, primarily, we’re looking at refractoriness to thalidomide ranging from 4% to 23%. It’s also important to look at their last line of therapy to see if they were refractory.
With all of that variability, it’s really hard to say that there is going to be 1 right regimen just by looking at the efficacy endpoints, which are summarized at the bottom of the table. First of all, the median follow-ups range from as short as 23 months to as long as 67 months. That’s going to affect the ability to detect whether or not a median overall survival has been reached. Then, when we look at the response rates, the triplet arms range from 78% to 93%, and the control arms range from 66% to 76%. When we start looking at the survival-based endpoint, which is the primary endpoint for most of these studies, the progression-free survival in the control armsince it’s the same regimen—should, hopefully, be pretty comparable. We can see it’s as low as 14.7 months for ixazomib and as high as 17.5 months. Although that difference may seem subtle, when we look at the relative value added of the novel therapy, a difference of 3 months could really make quite a difference in the value added of a novel agent.
One way to consider value added is through the hazard ratio, which I think we have not historically had to use in myeloma. There really weren’t that many choices to pick from. But, when we look at the hazard ratios, they range from as high as 0.74 to as low as 0.44. One of the standouts here is that the daratumumab/lenalidomide/dexamethasone regimen had the lowest hazard ratio0.44. This means almost a 60% improvement in progression-free survival with the addition of daratumumab. When we look at the overall survival, of course, again, because the median follow-ups are different, we’re not going to reach a median overall survival for some of these arms. But the 2 that have longer follow-ups have an important implication. Both showed that the overall survival was improved, whether it was with the addition of elotuzumab or carfilzomib—with hazard ratios of 0.78 and 0.79.
Why is that important? I think it tells us that in the relapsed setting, if you treat with more aggressive regimens, that could eventually translate into an overall survival benefit with the caveat, of courseas I alluded to earlier—that we have to be mindful of access to therapy. A lot of these phase III studies are done ex-US [United States]. They may not show an overall survival benefit in the US. But, be that as it may, with all of the caveats of phase III studies, I think these are very important results. We have a lot of options for patients. So, using evidence-based medicine, this patient did get daratumumab with lenalidomide and dexamethasone because she was lenalidomide naïve.
The problem, as we discussed in the last case, is that most US patients are getting lenalidomide maintenance, which basically eliminates the entire table that we just looked at. If you were refractory to lenalidomide maintenance, you would not have been eligible for any of those studies, so, it’s good to have options for PI backbone-containing regimens. Here, we’re looking at Vd [bortezomib/dexamethasone]containing regimens. These are all phase III studies, again, except for the elotuzumab trial. So, we have Vd as a control arm. In CASTOR, we have the addition of daratumumab. In ENDEAVOR, carfilzomib is used at 56 mg/m2. We know about the addition of panobinostat to Vd. Elotuzumab was looked at in the ELOQUENT study. Finally, recently presented were results of the OPTIMISMM studyPVd [pomalidomide/bortezomib/dexamethasone] versus Vd.
The sample sizes range from 152 in the phase II study to higher ones in the phase III setting. Again, we see variability in ISS stage, in ISS, and in lines of therapy. The refractoriness to a PI goes down significantly because of the control arm, which is Vd. Refractoriness to an IMiD, however, ranges. Some of the patients were refractory to lenalidomide because this was also open in the US but was not reported. And refractory to last line therapy also varies.
When we look at the efficacy endpoints, again, the median follow-ups range from as short as 15.9 months to as long as 37.5 months. In the control arm, the response rates are typically around 50% to 60%, and the triplet therapies or the Kd [carfilzomib/dexamethasone] regimen at a high dose of 56 mg/m2resulted in a response rate ranging from 55% to 85%. Again, the primary endpoint was progression-free survival, and we see that the control arm’s range was from as short as 6.9 months to as long as 9.4 months. I think this is important because one of the unique features of the daratumumab study is that the Vd was stopped after 8 cycles. Many people criticize that. Obviously, you’re going to stack the odds in favor of the triplet regimen. When you look at the numbers, remember that these studies were often giving Vd intravenously, twice weekly. We are seeing that it’s hard to give Vd for too long, either because of efficacy or tolerability. The range is from 7 months to 9 months, so it’s not that the daratumumab and Vd control arm is such an outlier as compared with the other arms.
When we look at the value added, again, we see a very striking hazard ratio benefit with the addition of daratumumabdown to 0.32. Again, all of the other ones also showed a favorable benefit—ranging from 0.53 to 0.72. I think using the hazard ratio is more justified. We can see, for example, that with the PVd/Vd control arm, we had a median of 2 lines of therapy in some of those patients. In some of these more heavily treated patients, we might not expect as much of a benefit, but the hazard ratio is telling us the value added. Again, when we look at the overall survival, the ENDEAVOR study has recently reported to translate into an overall survival benefit. The PANORAMA study did not show that benefit, but it is not currently used extensively in the US. The progression-free survival benefits can translate into overall survival, but, again, we have to remember the importance of drug access and the primary versus secondary endpoints.
Transcript edited for clarity.
Advertisement
Related Content







































Advertisement
Advertisement
Trending on Targeted Oncology - Immunotherapy, Biomarkers, and Cancer Pathways
1
Early CAR T Brings Questions of Preferred Bridging in Multiple Myeloma
2
Selinexor Plus Ruxolitinib Improves Spleen Responses, Shows OS Signal in Frontline Myelofibrosis
3
ASCO 2026 Breast Cancer Highlights: Beyond the LBAs
4
Phase 3 Trial of Sacituzumab Govitecan Plus Pembrolizumab Stopped Early in First-Line mNSCLC
5